
Abstract
Preliminary development of a fiber optic bilirubin sensor is described, where an unclad sensing portion is used to provide evanescent wave interaction of the transmitted light with the chemical environment. By using a wavelength corresponding to a bilirubin absorption peak, the Beer–Lambert Law can be used to relate the concentration of bilirubin surrounding the sensing portion to the amount of absorbed light. Initial testing in vitro suggests that the sensor response is consistent with the results of bulk absorption measurements as well as the Beer–Lambert Law. In addition, it is found that conjugated and unconjugated bilirubin have different peak absorption wavelengths, so that two optical frequencies may potentially be used to measure both types of bilirubin. Future development of this device could provide a means of real-time, point-of-care monitoring of intravenous bilirubin in critical care neonates with hyperbilirubinemia.
Introduction
Bilirubin is a normal breakdown product of hemoglobin. The liver conjugates this bilirubin with glucuronic acid to convert it into a water-soluble form, which is removed from the body via bile. Because the neonatal liver has not yet developed sufficient conjugation enzymes to keep up with bilirubin production, blood bilirubin levels typically increase temporarily after birth, but then return to normal within about a week. In some cases, blood bilirubin levels continue to increase (hyperbilirubinemia) to the point where bilirubin may enter the brain, resulting in kernicterus. Kernicterus causes irreversible brain damage, choreoathetoid cerebral palsy, mental retardation, sensorineural hearing loss, gaze paresis, opisthotonus, and death. Although it is more common in premature newborns, kernicterus can occur in full-term infants. 1 Kernicterus is completely preventable with prompt treatment, yet it continues to occur in the United States and elsewhere. Since the 1990s, kernicterus in full-term infants has reportedly re-emerged for reasons that are not entirely known. 2 Hyperbilirubinemia occurs in about 60% of all newborns, and approximately 80% of pre-term infants develop hyperbilirubinemia each year. In 2006, 12.8% of U.S. births were pre-term, representing a 21% increase since 1990. The bilirubin levels in pre-term infants tend to be higher, more persistent, and more likely to be associated with neurological injury than with term neonates. This increased intensity and duration, as well as immaturity of the blood–brain barrier, has led to concerns about greater risk of kernicterus in pre-term infants at much lower bilirubin levels than in healthy near term or term neonates. Over 90% of extremely low birth weight neonates (generally also pre-term) receive treatment for hyperbilirubinemia. 3
Current Methods of Bilirubin measurement
The most visible evidence of hyperbilirubinemia is jaundice (ie, yellow skin and sclera). However, skin measurements may be confounded by hypoperfusion and even normal dark pigmentation. 4 Furthermore, quantitative skin measurements typically underestimate blood bilirubin concentrations that exceed certain levels. Clinical assessment of the degree of jaundice by a physician examining the skin has been poorly correlated with actual serum bilirubin levels. 4 In neonates, bilirubin is currently measured in drawn venous blood samples (heel sticks) in the laboratory. This blood sample is transported to a laboratory and centrifuged to remove the cellular components. A spectrophotometer is then used to measure the bilirubin absorption in the liquid component of the blood. Even when ordered stat, the laboratory results may not be available for an hour. Bilirubin is present mostly in two forms in the blood: conjugated and unconjugated. There is evidence that unconjugated bilirubin better predicts neurotoxicity than total (ie, conjugated plus unconjugated) bilirubin concentration. 5 Current methods used to measure conjugated and unconjugated bilirubin concentrations require adding chemicals to the blood sample and making multiple measurements.
Concept of the Proposed Bilirubin sensor
While a fiber optic normally consists of an inner core and an outer cladding, this sensor requires an unclad region so that the evanescent portion of the transmitted light can interact with its environment outside the fiber (Fig. 1). When the wavelength of transmitted light corresponds to a bilirubin absorption peak, the amount of light absorbed can be related to the concentration of the bilirubin via the Beer-Lambert Law. Further details may be found in Babin. 6
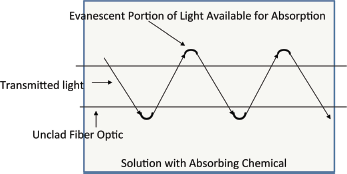
Concept of evanescent light absorption around an unclad fiber optic.
In this report, we describe a preliminary investigation to determine whether a fiber optic sensor may be used to measure bilirubin in high-risk neonates. Specifically, the experiments were designed to determine whether the evanescent portion of light immediately outside an unclad fiber optic would be sufficient for measuring bilirubin concentration by its absorption in the surrounding fluid. This investigation represents a first step in the eventual development of a fiber optic sensor that could be used to make in vivo measurements of bilirubin in the neonate.
The proposed sensor would be a simple multi-mode fiber optic that is unclad near the terminal end, where the terminal end would have a means of reflecting the light back up the fiber so that measurements could be made at the fiber end external to the infant. The difference in the measurements between the transmitted and returned light would be the amount of light absorbed by the bilirubin within the blood stream. The fiber optic sensor would be inserted by means of an intravenous line so the measurements would be of venous blood, the same type of blood measured currently with venipuncture. The following experiment is designed as a preliminary in vitro test of the principle that the bilirubin concentrations can be measured by this technique in a laboratory setting. Therefore, the fiber in these experiments does not have the reflective coating at the terminal end, so the measured absorption is based upon the difference between the light entering the fiber from the source and exiting the fiber at the measurement end (Fig. 2).
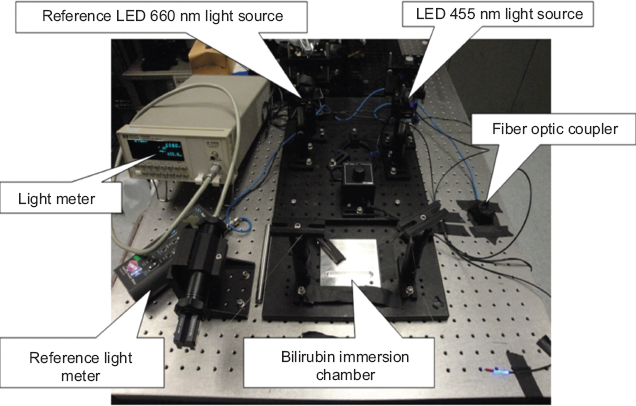
Photograph of the experimental arrangement.
Experimental
Materials
Plastic multi-mode optical fibers were provided by Lumitex, Inc. (www.lumitex.com). These fibers consisted of a polymethylmethacrylate (PMMA) core with a refractive index of 1.492 and a fluorinated polymer cladding with a refractive index of 1.402. The overall diameter was 250 μm, while the core diameter was about 245 μm. The numerical aperture of the fiber was 0.48-0.54, with 0.51 being typical. The fibers to be tested each had a 4 cm linear section of the cladding removed by a Lumitex proprietary mechanical process called Uniglo®.
Measurements of bilirubin concentration versus light absorption were made using liquid bilirubin samples (available only in conjugated form) purchased from Verichem Laboratories (www.verichemlabs.com). These solutions are manufactured with concentrations known to high accuracy in order to be used as standard references by medical laboratories to calibrate the spectrophotometers used to make bilirubin measurements. The manufacturer provides these liquid samples in concentrations ranging from 0.00 (ie, no bilirubin) to 30.0 mg/dL because these concentrations include the normal to high concentrations seen in hospital settings. Therefore, these conjugated bilirubin solutions were used as the calibration standard in our experiments.
A separate set of experiments was performed in order to compare the absorption spectra of conjugated versus unconjugated bilirubin. However, unconjugated bilirubin was only available in a freeze-dried form. To have a consistent spectral comparison of these two forms of bilirubin, freeze-dried calibrated samples of both types of bilirubin were purchased from Lee Biosolutions (www.leebio.com). These freeze-dried samples were reconstituted into liquid form using the instructions provided by the manufacturer.
Measuring Bilirubin Absorption versus concentration
The experimental setup (Fig. 2) was based upon a dual wavelength spectrometer approach that minimizes interference from scattering and unequal path lengths by using the sample as its own reference solution. 7 We used a blue LED source with a dominant wavelength of 455 nm. A red LED source (dominant wavelength of 660 nm) was used as a reference because bilirubin absorbs little or nothing at this wavelength. Our photodetectors were sensitive to 455 and 660 nm. We added a 50% fiber optic coupler to provide two paths for the LED emitted light. One path went from each LED through the coupler and then directly to a light meter. The other path differed by passing through the fiber optic sensor after exiting the coupler. In this way, the measurements take into account fiber losses when the fiber does not pass through the bilirubin samples. Figure 3 illustrates how the effects of the bilirubin on light absorption could reliably be determined because the reference beam with a relatively non-absorbing wavelength would account for any path differences and losses not attributable to the presence of bilirubin. We measured the 455 nm (blue) and 660 nm (red) transmittances through bilirubin relative to no bilirubin passage.
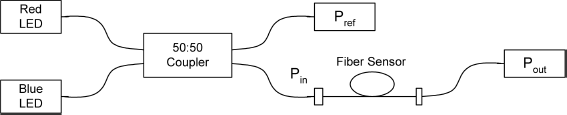
Schematic diagram of the experimental setup. P is the measured optical power at different locations in this diagram.
The equation for the ratio of these transmittances as a function of concentration was derived as follows. P is the power measured by an optical power meter. Because the 660 nm light (λred) is not absorbed by the bilirubin, we can measure the optical powers Pin and Pref to obtain a constant A using:

Transmittance is defined as the ratio of the power after transmission through the sample to the power entering the sample. Therefore, the transmittance through the sensor at 660 nm is then measured as:

Similarly, assuming the blue light (λblue) is absorbed by the bilirubin, we can measure Pin and Pref to obtain a constant B using:

The transmittance through the sensor at 455 nm is then measured as:

These transmittances are related to the absorption coefficient α for the fiber and to the molar absorptivity ε for the solution), the bilirubin concentration C, and the optical path length L:


Finally, taking the ratio of the transmittances gives:

Measurements can be used with equations (1)–(4) to determine the ratio on the left-hand side of (7). Equation (7) can then be used to derive a relationship between this ratio and known concentrations C.
Measuring Conjugated versus Unconjugated Bilirubin Absorption peaks
To compare the absorption peaks of conjugated versus unconjugated bilirubin, we made measurements of their absorption spectra using a dual beam Perkin Elmer Lambda 950 spectrophotometer at wavelengths from 190 to 900 nm (covering both visible and ultraviolet). The manufacturer provided highly purified conjugated and unconjugated bilirubin in freeze-dried form, including specific instructions for reconstituting the bilirubin into liquid solution. Therefore, the unconjugated bilirubin was reconstituted using 0.1N NaOH solution, while the conjugated bilirubin was reconstituted in deionized water. The final concentrations of conjugated and unconjugated bilirubin were both 5 mg/dL so that the absorption peak intensities would be comparable. This concentration is also near the low end of the abnormal range for bilirubin. The dual beam spectrophotometer enabled comparison of the absorption from the unconjugated and conjugated bilirubin with NaOH and deionized water solutions, respectively. Using this dual beam technique, the spectrophotometer subtracted the corresponding absorption by these solvents to give the absorption spectrum for each bilirubin species alone.
Results
Bilirubin Absorption versus Concentration measurements
The goal of these measurements was to determine the coefficients of a relationship between bilirubin absorption and concentration for comparison with that derived by Doumas et al, 8 who made the measurements directly in human serum samples without using fiber optics. Doumas et al 8 experimentally derived a linear relationship between absorption and concentration of unconjugated bilirubin with a slope of 0.000769 and an intercept of −0.0003, for concentrations in mg/dL. After making 40 absorbance measurements, we found that the relationship between evanescent absorption and bilirubin concentration was very linear (R2 correlation of 0.95). These data could be approximated by absorbance = 0.0008 * (concentration in mg/dL) −0.0005. This result shows that our experimental results using a fiber optic were consistent with Doumas et al 8 and with the Beer–Lambert law. Therefore, this is evidence that bilirubin concentration could be measured using evanescent wave absorption.
The measured ratio of optical transmittances at 455 nm to 660 nm versus bilirubin concentration was then fit to an exponential equation to determine the constants for equation (7):

To investigate these discrepancies, we observed the unclad portion of this fiber under a microscope while illuminating one end with a white light LED. From the photomicrograph in Figure 4, the white light is seen exiting the fiber from the areas where the cladding has been successfully removed. The darker segments along the edges of the fiber are where cladding remains attached to the core. We therefore believe that this incomplete cladding removal was primarily responsible for the relatively weak response of the sensor.
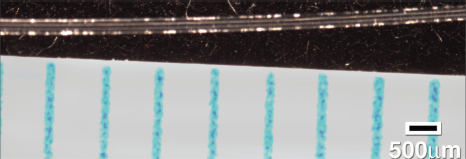
Photomicrograph of fiber illuminated by white light showing areas along the fiber where the cladding had been removed so that the light could leave the fiber. Note the ruler in the lower right indicating the scale in μm. The overall (core plus cladding) fiber diameter is 250 μm.
If we had been successful in removing more cladding, it is conceivable that the measured equation (8) might have been closer to equation (7). However, repeated attempts to remove more cladding using ethylene acetate, as described in Angelini et al, 10 always resulted in fiber breakage. Further work is needed to determine a better method to accomplish more complete cladding removal so that these fibers can again be tested.
Measurement of Conjugated versus Unconjugated Bilirubin Absorption peaks
Figure 5 shows the absorption spectra for conjugated and unconjugated bilirubin over the range from 250 to 600 nm. The concentrations of both species were 5 mg/dL in order to make comparable measurements. Hyperbilirubinemia is defined as a total bilirubin concentration greater than 5 mg/dL. The unconjugated bilirubin had peaks at about 220 and 425 nm. The conjugated bilirubin had peaks at about 190 nm and 455 nm. Therefore, in principle, one may be able to use a fiber optic sensor to measure these two forms of bilirubin. For example, one could use a tunable laser or LEDs with bandpass filters, along with signal processing algorithms such as those that perform spectral fitting, in order to distinguish, for example, the absorption at the 425 versus 455 nm peaks.
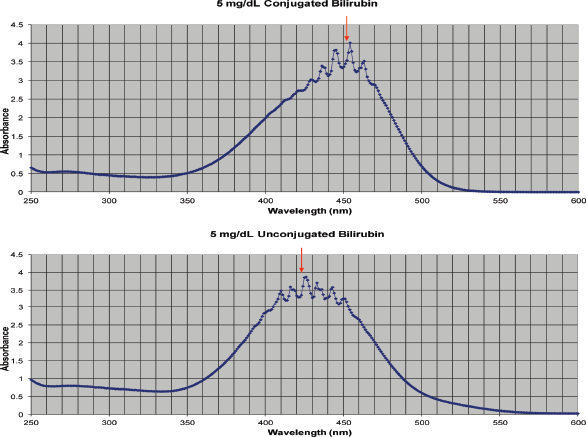
Absorption spectra of conjugated (top) and unconjugated (bottom) bilirubin. The arrows point to the approximate centers of the absorption peaks. The concentration of each solution was 5 mg/dL
Discussion
The experiments described herein were meant to determine whether absorption of the evanescent light external to a simple unclad multi-mode fiber optic could be related to bilirubin concentration in the surrounding fluid. If the absorption of evanescent light by a chromophore in its liquid chemical environment behaves in a similar manner as bulk absorption, then a fiber optic sensor could be used to measure the concentration of the chromophore having an absorption peak at that light frequency. While incomplete cladding removal likely resulted in less than optimal sensitivity of the sensor to absorption, there was enough of a response to show consistency with the Beer–Lambert Law and the results of Doumas et al.8,9
The diameter of the fiber used in these experiments would fit inside 24-26 gage intravenous needles, thereby allowing real-time, point-of-care monitoring of bilirubin levels. If needed, smaller diameter multi-mode optical fibers could in principal be used and would actually provide more evanescent wave interaction. A reference wavelength of 660 nm was used because bilirubin shows little or no absorption here. The dominant chromophore in human blood is the hemoglobin found mostly in erythrocytes. Because the absorptivity of hemoglobin falls dramatically above 600 nm, 11 using 660 nm measurements as a reference would likely not be impacted by the presence of hemoglobin. However, if 660 nm proves not to be a good reference when the fiber optic is tested in blood samples, a higher wavelength could be used. The wavelengths of light used in these experiments have no known harmful effects. The light would remain within the fiber until it reaches the sensing end. The sensor does not require high light intensities in order to make the absorption measurements.
As mentioned previously, measuring both the conjugated and unconjugated components of bilirubin could be beneficial. 5 The measured absorption spectra of the unconjugated and conjugated species of bilirubin suggest that the spectral features are unique and that some type spectral fitting and processing routines, perhaps using a tunable laser, could be used to measure these components separately.
Need for a New Method of Bilirubin measurement
Neonates identified with hyperbilirubinemia are typically monitored by one or more daily heel sticks to obtain blood levels. Cumulative drops in blood volume from these heel sticks may become a concern in premature neonates due to their impact on other factors associated with prematurity. 12 However, heel sticks remain the current standard for such measurements. Even so, there are cases in which this monitoring failed to detect rapid rises in bilirubin levels, leading to infants developing irreversible brain damage before more aggressive therapy could begin [eg, Bertini et al]. 13 According to the American Academy of Pediatrics (AAP) Subcommittee on Neonatal Hyperbilirubinemia, the root causes of kernicterus include underestimating the severity of jaundice and delay in measurement. 14 Accordingly, there remains a need for an improved method and device for high-risk patients that allows for real-time, point-of-care monitoring of bilirubin levels in venous blood.
The standard treatment for hyperbilirubinemia is phototherapy, which exposes the infant to special lighting to break down the skin bilirubin. As this skin bilirubin breaks down, bilirubin may continue to be deposited in the skin until the blood levels return to near normal, so there may be some delay in lowering blood levels. Phototherapy risks include overheating, eye damage, and keeping the infant in isolation during therapy. In more urgent and severe cases, exchange transfusion is used. Exchange transfusion involves the complete removal and replacement of blood, and risks include heart and lung problems. There is a need to balance the risk of kernicterus with the potential adverse consequences of therapy. Having a new in vivo real-time method for bilirubin measurement and monitoring during phototherapy would provide a substantial benefit for these patients, including earlier initiation of therapy to prevent neurological damage and earlier termination of therapy once blood bilirubin levels return to normal. Some studies have suggested that unconjugated bilirubin better predicts neurotoxicity than total (ie, conjugated plus unconjugated) bilirubin concentration. 5 Therefore, an in vivo sensor that measures both types of bilirubin may be useful. By being able to monitor closely and exactly the bilirubin levels both before and during phototherapy, irreversible adverse consequences may be avoided.
Future Work needed
Although the experiments described above are preliminary in vitro investigations, our results support the concept behind making absorption measurements using the evanescent portion of light with the peak absorption wavelength. To move forward in the development of this sensor, a technique must be found for completely removing the cladding without breaking the fiber. In addition, a reflective terminal end must be developed for the fiber to be used in vivo. Once these next steps have been accomplished, fiber sensors may be further developed for testing in blood, including animal studies. Following successful animal studies, rigorous review and approval would be required for studies in humans.
The real-time, point-of-care sensor proposed herein could significantly reduce delays and inaccuracies in current measurement technology, and may eventually allow for automated control of phototherapy. Rising bilirubin levels may be immediately addressed instead of waiting for laboratory results from the most recent heel stick. There would be less concern about pain and decreases in blood volume of low birth weight neonates from repeated heel sticks. In neonates being treated with phototherapy, earlier detection of a return to normal bilirubin levels may mean earlier return of the infant to the mother. Therefore, further development of this technology could prove beneficial in bilirubin monitoring of premature infants in critical care.
Author Contributions
Conceived and designed the experiments: SMB and RMS. Analyzed the data: SMB. Wrote the first draft of the manuscript: SMB. Contributed to the writing of the manuscript: SMB and RMS. Agree with manuscript results and conclusions: SMB and RMS. Jointly developed the structure and arguments for the paper: SMB and RMS. Made critical revisions and approved final version: SMB and RMS. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
We would like to express our sincere appreciation for the efforts of Jill LaFavors and the late Ed Ott, who provided valuable assistance in the measurement of bilirubin absorption spectra and the photomicrography of the sensor. We also appreciate the generosity of Lumitex, Inc., for providing us with the optical fiber used in these experiments.