
Abstract
Background:
Coronavirus disease 2019 (COVID-19) virus has caused widespread Acute Respiratory Disease globally since 2020. Patients with evidence of lower respiratory illness either clinically or radiologically had moderate-to-severe illness. COVID respiratory and nonrespiratory symptoms (psychological and cognitive) noticed after 4–8 weeks of primary disease were called long COVID syndrome. Survivors of moderate-to-severe disease had a poor quality of life. The main objective of this retrospective study was to assess the role of outpatient pulmonary rehabilitation (PR) done in moderate-severe COVID-19 survivors who had symptoms after 4–8 weeks at Shaivam Lung Rehabilitation Centre, Ahmedabad.
Methods:
We analyzed the impact of PR on 30 patients' post-COVID-19 who were willing to participate during the ongoing pandemic. It was an outpatient 6–8 weeks of program designed to target respiratory and general muscle training, relaxation technique, nutritional counseling, occupational and psychological support. Patients were tested with of combination of self-assessment quality of life scale (adapted from short form 36 questionnaire), muscle training, dyspnea scale, and physical assessment. The standard objective assessment included oxygenation index (SpO2/FiO2 ratio), 6 min walk distance (6 MWD), Modified Medical Research Council (MMRC) score, manual muscle testing (MMT) along with pulmonary function testing. All these subjective and objective variables were tested pre- and post-PR program to assess the impact on defined parameters.
Results:
From December 2020 to March 2022, we studied the impact of PR on 30 out of 55 patients fitting into the inclusion criteria. Significant benefit was noted in subjective Short Form 36 (SF 36) score and objective (6 MWD, MMRC, oxygenation, MMT) quality of life post-PR program (P < 0.001). Improvement in spirometry was not statistically significant, indicating structural chronicity of COVID pulmonary fibrosis.
Conclusion:
PR is safe, effective, and feasible on an outpatient basis in COVID-19 survivors of illness with poor quality of life. Further research is required to prove its widespread benefit in such patients.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) a novel Betacoronavirus, was responsible for the Global outbreak of acute respiratory illness known as coronavirus disease 2019 (COVID-19). Manifestations of COVID can be mild to moderate in 80% of cases, 15% have severe disease, and 5% have a critical illness.[1],[2] Those needing oxygen therapy or in need of critical care services have guarded outcomes. The disease causes major alveolar damage, severe inflammation, and vascular insult resulting in hypoxemic acute respiratory failure. Moderate-to-severe cases require oxygen therapy or mechanical ventilation. Long COVID syndrome exists in patients who manifest symptoms even after 4–8 weeks of primary disease.[3] Physical, psychological, and cognitive impairment is seen in such patients after recovery.[4] Intensive care unit survivors have a poor quality of activity of daily living due to the high prevalence of muscle weakness and physical performance impairment.[5]
COVID pulmonary fibrosis is a sequelae of severe COVID-19 lung disease.[6] In the perspective of functional medicine, it reduces both the motility and mobility of organ and locomotion respectively. In such patients, therapeutic dilemma hounds around the treating physician and no proven benefits have been seen with existing medications.
Pulmonary rehabilitation (PR) is defined as a comprehensive intervention based on a thorough patient assessment followed by patient-tailored therapies that include but are not limited to, exercise training, education, and behavior change, designed to improve the physical and psychological condition of people with chronic respiratory disease and to promote the long-term adherence to health-enhancing behaviors. This nonpharmacological intervention is known to decrease symptoms (dyspnea and fatigue), improve exercise tolerance and quality of life, reduce health-care utilization, as well as increase physical activity among such patients.
PR has been the main therapeutic intervention in lung diseases such as chronic obstructive pulmonary disease (COPD), interstitial lung disease, pulmonary hypertension, and advanced asthma. Extrapolating its benefit on quality of life it has been recommended in acute and subacute lung disease. Along with reducing dyspnea and fatigue, PR improves exercise endurance and many areas of health-related quality of life. Such personalized treatment plans can reduce complications, enhance endurance, social participation, and reduce the medical budget.[7],[8],[9],[10],[11]
PR has been proposed by National/International guidelines and recommendations.[12],[13] Our study aimed to report the safety, functional outcome and preserve lung function with PR in subjects suffering from COVID-19 sequelae.
Methods
Study design
This retrospective observational study screened patients of post-COVID-19 undergoing outpatient PR at Shaivam Lung Rehabilitation Centre, Ahmedabad, from December 2020 to March 2022. Patients from both the waves of COVID-19 were included to study the impact of the structural and functional impact of different strains. Chest specialist and PR specialist manage this center. Ethics Committee Clearance was taken (AHD/ACD-018/09-20).
Inclusion criteria for rehabilitation were based on the following criteria
Willingness to undergo outpatient PR during the pandemic
4–8 weeks post-COVID (no active illness)
Oxygen requirement <2 L/min (LPM)
Age between 18 and 70 years
No ongoing indoor treatment
Hemodynamically stable
No active cardiac, neurological, or nephrology disease
Mental stability to undergo a rehabilitation program.
Exclusion criteria
Noncooperative and mentally unfit
Right heart failure
Those who could not complete the rehabilitation session due to personal or epidemic-related travel restrictions
Persistent reverse transcriptase polymerase chain reaction (RT-PCR) positive
Lung transplant candidate
Medically deemed unstable due to active cardiorespiratory, nephrology or neurological disease.
Intervention
Retrospective data of all patients who underwent rehabilitation were studied. Data were collected in regard to Past Medical Diseases, ongoing therapeutics, and detailed rehabilitation program impact. Those who could complete 6 weeks of PR program, were enrolled finally for study. Data were entered and analyzed using Microsoft Excel. Paired t-test was used to assess statistical significance. Subjects were free to withdraw consent during the participation period for any personal or pandemic-related lockdown reasons. Post-COVID physical limitation was assessed by 6 min walk distance (6 MWD), chest expansion, and symptoms on exertion. Baseline quality of life was judged by Short form (SF-36) questionnaire which assesses eight health concepts based on physical functioning, physical role, pain, general health, vitality, social function, emotional role, and mental health [Supplementary File 1].[14],[15]
Our PR program was according to the Italian Position Paper.[13] Type, intensity, timing, and modality of intervention were tailored to individual patients as disease, tolerance, and oxygen requirement. Only patients with RT-PCR tests for SARS-CoV-2 were included in our study. Infection control practices were strictly followed during the entire rehabilitation program.
Manual muscle testing (MMT) was used to determine the extent and degree of muscular strength/weakness resulting from disease, injury, or disuse.[16] Subjective breathlessness was assessed by the Modified Medical Research Council (MMRC) score.[16],[17] Need of oxygen was assessed along with the dose of oxygen (in LPMs) pre- and post-rehabilitation. We looked for nature and quality of cough along with the breathing pattern. Chest expansion was studied by taking the measurement at deep inspiration and expiration by measuring tape at the level of the intermammary line. Normal range of motion is about 2.5″ which is limited in restrictive lung diseases. Chest mobility was assessed as per the American Thoracic Society (ATS)/European Respiratory Society (ERS) task force statement.[18] Pulmonary function testing (PFT) such as 6 MWD and PFT was tested in all patients pre- and post-PR. Apart from this standard post-COVID radiology, routine laboratories and Echo were reviewed as and when required. Baseline and/follow-up computed tomography (CT) Chest and diffusion capacity of lung for carbon monoxide (DLCO) were not available in all patients hence were not studied in our study.
Core PR included endurance training, strength training, respiratory physiotherapy, relaxation technique, occupational therapy, and psychological and nutritional support [Supplementary 2]. After completion of PR therapy, they were guided for home-based further programs.
A descriptive statistics were conducted for all the continuous variables and proportions for the categorical variables. The pre–post comparison was conducted based on the two-sample t-test with unequal variances and significance level was considered with P < 0.05. All the analyses were conducted in STATA 14.1. (StataCorp LP. 2015. Stata Statistical Software, College Station, TX).
Results
Of 55 patients screened, 30 were taken for this retrospective Observational study. Sixty percent of them were male and 40% were female. Patient's age distribution is given in [Table 1]. Eighty-six percent of patients had associated comorbidities along with COVID-19 lung disease.
Age-wise distribution across genders among studied participants

In our study, majority of the patients were above 40 years of age. Eighteen patients were male and 12 were female [Table 1]. Among 30 patients, 6 had mild, 14 had moderate, and 10 had severe COVID-19.
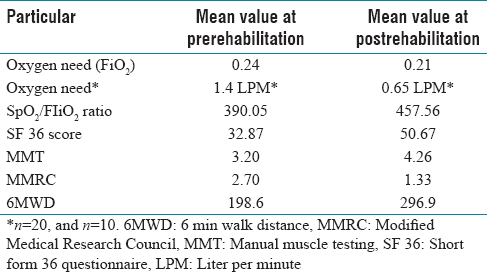
[Table 2] emphasizes that, 20 patients (66%) were having oxygen therapy at the time of enrolment. A significant impact of rehabilitation was seen in oxygen need (P value). SF 36 score, MMT, MMRC, and 6 MWD.
Basic profile of participants compared with pre- post-intervention
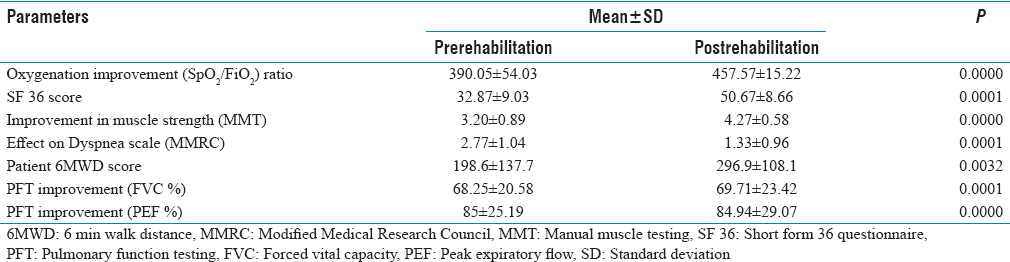
While comparing the pulmonary function indicators as pre–post rehabilitation, most of the parameters indicated statistically significant improvements as shown in [Table 3]. The mean oxygenation improvement was observed from 390.05 ± 54.03 to 457.57 ± 15.22 in the postrehabilitation. Similarly, the mean SF score improved from 32.87 ± 9.03 to 50.67 ± 8.66. The mean MMT score was observed to be improved by 1.07, increasing from 3.20 ± 0.89 to 4.27 ± 0.58. In contrast, the effect on the dyspnea scale, i.e., MMRC score decreased from 2.77 ± 1.04 to 1.33 ± 0.96. Similarly, there were minimal changes were observed in PFT values, forced vital capacity (FVC%) improved from 68.25 ± 20.58 to 69.71 ± 23.42 and peak expiratory flow (PEF%) declined from 85 ± 25.19 to 84.94 ± 29.07.
Comparison of pulmonary function indicators pre- post-intervention
Discussion
Those who survive COVID-19 illness can still have symptoms and signs due to significant structural and functional limitations in terms of dry cough, variable grades of dyspnea, chest pain, and poor appetite along with a lack of ability to perform day-to-day activity. Long COVID syndrome is now a defined entity.[4] COVID-19 fibrosis is well known to affect quality parameters in survivors.[18]
In our study, improvement was seen in SF score with PR. Statistically significant benefit was seen in the pre- versus post-rehabilitation score of all patients. The quality of life as adjudged by SF 36 was better in postrehabilitation phase indicating a value-added intervention in such patients who are left to nature and some experimental therapies to improve after such a nasty viral insult. This correlates well with findings published in the indoor rehabilitation work published by Gloeckl et al. among 50 patients studied.[2] The mean score improved from 32.87 to 50.67 with a P < 0.0001. The improvement seen with outpatient PR program in post-COVID-19 correlated well with their objective and subjective quality of breathing, respiratory mechanics, and activity of daily living.
The 6 MWD, a measurable parameter of lung function also showed statistical significance from 198.6 to 296.9 m (P = 0.0001). 6 MWD has been a gold standard of testing in various chronic lung disease patients for the benefits of PR.[19],[20] Even the ATS and ERS coordinated international task force for COVID-19 have recommended testing for hypoxia at rest and exertion on discharge. Similar testing is recommended at the end of 6–8 weeks of PR program.[12] The significant improvement in 6 MWD is a robust boost to experience the physical and mental strength.
MMRC dyspnea score has been studied extensively in COPD patients.[21] MMRC has been an integral part of our questionnaire which showed statistically significant impact in post-PR patients (2.77–1.33). This along with 6 MWD makes the effectiveness of our rehabilitation program significant. Oxygenation improvement noted in our study is a significant finding highlighting the importance of chest wall and diaphragm wall contribution to respiratory physiological improvement. Ten patients (33%) were weaned from oxygen postrehabilitation.
MMT score a surrogate for muscle strength also showed improvement with a robust PR program (3.2 in pre- vs. 4.28 in postrehabilitation). Strengthening exercises used were with the aid of theraband, hand and leg cycle along with IT band mobilization.
Health-related quality of life can be defined as “the gap between our expectations of health and our experience of it.”[22] A primary aim of the treatment of lung diseases is to enhance the quality of life by reducing the impact of the disease. However, the relationship between symptoms and exercise capacity, or functional limitation and quality of life, is neither simple nor direct. Apart from SF 36, other questionnaires which have been used in lung disease assessment are Chronic Respiratory Disease Questionnaire,[23] St George's respiratory Questionnaires.[24],[25] and EXACT-respiratory symptoms tool.[26] SF 36 also assesses the impact on nonrespiratory organs which is not uncommon to COVID-19; our positive impact can be generalized.
Kunoor et al. have documented function and psychological benefits post-COVID-19 PR from their single-center experience.[27] Short-term effects of outpatient PR were documented in a systemic review for COVID-19 by Cochrane group.[28]
We could not demonstrate statistical significance in PFT parameters studied (PEF rate and FVC). DLCO was not studied as more than 70% of patients enrolled did not have baseline tests available or could not perform the procedure physically. The lack of improvement noted in spirometry is explained due to the time needed to regress or reverse the structural changes in post-COVID Pulmonary Fibrosis patients. Reversal of COVID-19 fibrosis is unpredictable and time to achieve normal lung function has not been studied so far.[29],[30] Due to cost constraints, follow-up CT chests were not studied. The findings in our study emphasize careful monitoring of Lung function on subsequent follow-up of such patients.
Jiandani et al. have already published Evidence-based Indian Consensus in 2020 for acute therapy in COVID-19 patients.[31] In general, we have demonstrated that outpatient PR program for moderate-to-severe COVID-19 survivors having poor quality of activity of daily living decreases dyspnea and improves exercise capacity and measurable parameters of quality of life. A study by Wang et al. concluded that given the possibility of long-term disability, outpatient posthospitalization PR may be considered in all patients hospitalized with COVID-19.[32]
Limitations of the study
Due to outpatient nature of assessment, we could not take immediate survivors post-COVID who were bedridden. The sample size during the ongoing COVID pandemic was small limiting the statistical validity across the spectrum of illness. We could not do a prospective study due to COVID-19 pandemic. Underlying comorbidity were not studied as confounding factors due to the small sample. Radiological inclusion criteria were not taken due to a lack of evidence in post-COVID-19 for disability. Due to resource limitations, follow-up CT scans are not available for comparison of disease sequelae. We only assessed short-term effects (6–8 weeks) of PR. Given the heterogenicity of treatment in post-COVID survivors, we have not studied the impact of pharmacological agents on recovery.
Conclusion
Barman et al. have highlighted the dire need of studies for clinicians to choose the best type of rehabilitation program and its effect.[33] Respiratory rehabilitation can improve exercise capacity and PFT parameters in patients recovering from SARS infection. Our study has shown the impact of PR, its effectiveness in patients recovering from moderate to severe COVID-19 infection, including those requiring assisted living or oxygen therapy. Literature is widely available for positive effect of rehabilitation in different lung diseases.[34]
We have shown that targeted PR is safe and effective in patients' post-COVID-19 illness to improve the physical and functional recovery. It will act as a guide to build a robust rehabilitation program in survivors of COVID-19 and similar disabling diseases of the lung. The results are in sync with existing literature for COVID-19 rehabilitation effect across the globe and chronic lung disease. Such positive impact of PR in moderate-to-severe COVID-19 survivors should be cumulatively assessed and standardized protocols formulated to update the existing therapeutic guidelines.[35]
Supplementary Files
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We would like to thank Dr. Jinal Prajapati, Dr. Digna Rana, Dr. Dhruvi Devda, Mr. Chirag Parmar, and Ms. Mittal Dave (Team Shaivam Clinic).
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
IEC number AHD/ACD 018/0920.
Funding
Nil.
Author's contribution
Dr. Manoj K Singh: Introduction, conceptualisation, data analysis, conclusion. Dr. K M Annamalai: Scoring methodology, rehabilitation protocol, consolidating follow up during COVID pandemic times.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.