
Abstract
Aim:
Culture-negative sepsis (CNS) is a common but understudied entity. The objective of this study was to compare the incidence, characteristics, and outcomes of CNS with culture-positive sepsis (CPS).
Methods:
This was a prospective observational study of patients admitted to the medical intensive care unit (ICU) of a tertiary hospital from January to December 2015 with clinical suspicion of severe sepsis as defined by Consensus Conference Criteria 2001.
Results:
Patients with severe sepsis (n = 122) were studied of whom 66 (54%) were CPS and 56 (46%) were CNS. Patients with CNS had fewer comorbidities (0.7 ± 0.70 vs. 2 ± 0.8, P < 0.01). At presentation, CNS patients had less tachycardia (heart rate 92.5 ± 10.5 vs. 105.9 ± 13.2, P < 0.01), lower white blood cell counts (11859 ± 4791 vs. 14224 ± 3898, P = 0.003), lower need for vasopressors (38% vs. 68%, P < 0.01), and mechanical ventilation (23% vs. 53%, P < 0.01) compared to patients with CPS. The number of antibiotics on admission was similar between the groups (1.5 ± 0.6 vs. 1.6 ± 0.6, P = 0.36) but the duration of antibiotics was less in CNS (7.6 ± 1.7 days vs. 10.4 ± 2.6 days, P < 0.01). CNS had lower duration of ICU stay (6 ± 2.1 days vs. 7.8 ± 3.7 days, P < 0.01) and lower ICU mortality (7.1% vs. 22.7%, P = 0.02).
Conclusion:
CNS is very common in ICU. CNS patients compared to CPS tend to be less sick at presentation utilizing less resources but were initiated on a similar number of antibiotics on admission although for a shorter duration. Patients with CNS had a lower mortality in comparison to those with CPS.
Introduction
Severe sepsis is defined as a life-threatening organ dysfunction caused by a dysregulated host response to infection. Mortality is 30%–60% with rates increasing linearly according to the severity of sepsis despite advances in treatment modalities.[1] Bacteria are the most common causative microorganism in sepsis. Failure to administer early appropriate antibiotics increases mortality.[2] Cultures are positive in only 50% of patients and may lack sensitivity but earlier studies have inferred that the severity of illness and mortality were not significantly affected by microbiological documentation of sepsis.[3] There is less data on sepsis for which etiologic agents are not found. The medical literature is surprisingly devoid of information about rates of culture-negative sepsis (CNS) and outcomes of patients with CNS in India.
The aim of the study was to compare the incidence, characteristics, and outcomes of CNS with CPS.
Methods
This is a single-center prospective observational study of patients admitted to the medical intensive care unit (ICU) of a tertiary hospital from January to December 2015 with clinical suspicion of severe sepsis as defined by Consensus Conference Criteria 2001. The 2001 Consensus Statement defined sepsis as a host's inflammatory response to infection. Severe sepsis was defined as sepsis complicated by organ dysfunction. Exclusion criteria were age <18 years, prior antibiotic exposure (<90 days), and noninfectious mimics. Noninfectious mimics of sepsis include pancreatitis, drug overdose, and connective tissue disease. Two sets of blood cultures, each with an erobic and anerobic bottle, were drawn with an average volume of 10 cc per culture bottle.
The following data were collected: demographic characteristics, comorbidities, admission vitals, need for vasopressors, mechanical ventilation, provisional diagnosis made by the treating physician at the time of presentation, microbiological data, and the number and duration of antibiotics given based on the provisional diagnosis. Outcomes including ICU length of stay, ICU mortality, antibiotic utility, rates of de-escalation, and the final diagnosis at discharge were recorded. Categorical variables are reported as percentages and continuous variables as mean and standard deviation. For the comparison of groups and proportions, Pearson's correlation analysis, t-test, and Chi-square tests were used. Statistical software SPSS version 20.0 (SPSS, IBM, USA) was used.
Results
One hundred and twenty-two clinically suspected severe sepsis patients were studied of which 66 (54%) were CPS and 56 (46%) were CNS. Characteristics between the groups were compared using Standard t-test. The mean age of the patients studied was 63 ± 14 years and 60 (49.1%) patients were male. CNS was seen more in females compared to males (42% vs. 60%, P < 0.05) [Table 1].
Demographic characteristics of patients

At presentation, CNS patients had fewer comorbidities (0.7 ± 0.7 vs. 2 ± 0.8, P < 0.01), had less tachycardia (92.5 ± 10.5 vs. 105.9 ± 13.2, P < 0.01), lower white blood cell (WBC) counts (11859 ± 4791 vs. 14224 ± 3898, P = 0.003), lower need for vasopressors (38% vs. 68%, P < 0.01), and mechanical ventilation (23% vs. 53%, P < 0.01) [Table 2].
Characteristics of patients on admission

The number of antibiotics on admission was similar between the groups (1.5 ± 0.6 vs. 1.6 ± 0.6, P = 0.362) but the duration of antibiotics was less in CNS group (7.6 ± 1.7 days vs. 10.4 ± 2.6 days, P < 0.01). De-escalation of antibiotics was considered after the final culture reports if the initial broad-spectrum cover was appropriate and antibiotics were narrowed to the specific organism but to a lower spectrum of antibiotics. In our study, de-escalation of antibiotics was seen in 20 patients of the CPS group (30%), whereas 38 of the CNS group (68%) had the same antibiotic continued despite culture negativity [Figure 1].
Antibiotic usage after culture and sensitivity report. CPS: Culture-positive sepsis, CNS: Culture-negative sepsis

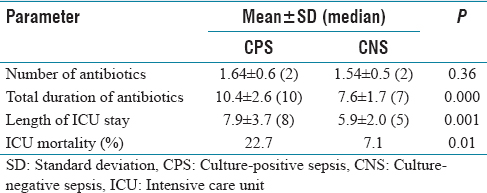
CNS had lower duration of ICU stay (6 ± 2.1 days vs. 7.8 ± 3.7 days, P < 0.01) and lower ICU mortality (7.1% vs. 22.7%, P = 0.02) [Table 3].
Antibiotic usage and outcomes of patients
Discussion
CPS is defined as severe sepsis with a microbiological evidence of infection, whereas CNS is severe sepsis without a microbiological evidence of infection in an appropriate culture specimen. In our study of the 122 clinical suspected severe sepsis patients, 54% were CPS and 44% were CNS. This shows that CNS is present in almost half of the ICU patients with severe sepsis admitted to the ICU. Our incidence of CNS is similar to a large study conducted by Gupta et al. in which of the 6,843,279 admissions with severe sepsis, 3,226,406 (47.1%) had culture-negative sepsis.[4] Causes for CNS are lack of sensitivity of C and S, prior antibiotic exposure, sampling error (insufficient volume and poor transport), slow growing/fastidious organism, low organism load (failure to capture in C and S), nonbacterial sepsis, and noninfectious mimics.[5] In our study, care was taken not to include patients with prior antibiotic exposure and noninfectious mimics, and samples were collected with the standard aseptic protocol. The results suggest that using only microbiological documentation of infection by cultures and sensitivity (gold standard) is insufficient to label an infection.[6]
Our study found that patients with CNS had fewer comorbidities, less tachycardia, and lower WBC counts. A study by Phua et al. in a large prospective cohort study of patients (n = 1001) presenting with severe sepsis also found an incidence of CNS in 41.5% of the cohort, with these patients presenting with less comorbidities and organ failure.[7] However, in their study, the identification of a pathogen was not independently associated with mortality. This may suggest that although CNS may be less severe compared to CPS, the clinical presentation is largely the same. In this study, a smaller percentage of CNS patients utilized similar resources with respect to the need for vasopressors (38% vs. 68%) and mechanical ventilation (23% vs. 53%) re-emphasizing the fact that CNS and CPS indistinguishable at presentation.
With respect to the utilization of antibiotics, we found in our study that the initial number of antibiotics started by the treating physician based on the provisional diagnosis was no difference between the two groups (1.54 ± 0.55 vs. 1.64 ± 0.61, P = 0.362) but the duration of antibiotics was less in CNS (7.57 ± 1.7 days vs. 10.4 ± 2.57 days, P < 0.01). Initial antibiotic therapy is usually chosen to broadly cover likely organisms causing the infection after incorporating the risks for resistant organisms and local susceptibility patterns. It is hence expected that the number of initial antibiotics used is similar between the two groups. Moreover, we excluded patients with antibiotic exposure within the previous 90 days making our patient cohort less heterogeneous. On day 5, after the final C and S report, it was also seen that 68% of the CNS group had the same number of antibiotics continued despite culture negativity. This could be because either the patient did not clinically improve or the physician wanted to complete the course of antibiotics despite negative cultures. When cultures are negative, risks of prolonged antibiotic duration often have to be balanced against the risk of sepsis flaring up after stopping antibiotics. The overall tendency among physicians is to continue the use of antibiotics adding to the cost and development of antibiotic resistance.[8]
It is likely that, patients with CNS had less severe disease in terms of needing organ support leading to subsequent shorter duration of ICU stay (6 ± 2.07 days vs. 7.8 ± 3.66 days, P < 0.01) and lower ICU mortality (7.1% vs. 22.7%, P = 0.017). We did not collect the data for possible etiologies of noninfectious causes of fever and we acknowledge that this could be a limitation of our study.
Conclusion
Culture-negative sepsis is very common in ICU. CNS patients compared to CPS tend to be less sick at presentation, utilizing less resource but requiring a similar number of antibiotics on admission although for a shorter duration. However, antibiotic de-escalation was not commonly practiced in CNS and optimal implementation of antibiotic de-escalation in CNS requires further evaluation.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Funding
Nil.
Author's contribution
Dr. Varun Byrappa: Data collection, data discussion, data analysis, and preparation of manuscript, Dr. Ramesh Venkataraman: Study concept, study design, data analysis monitoring, and preparation of manuscript, Dr. Nagarajan Ramakrishnan: Data analysis monitoring and manuscript approval, and Dr. Ashwin Kumar Mani: Data discussion, data analysis monitoring, preparation of manuscript, and manuscript approval.