
Abstract
Introduction
The prevalence of obesity in the United States is up to 40% in adults. Obese patients with severe sepsis have a lower mortality rate compared with normal body mass index (BMI) patients. We hypothesized that trauma patients with severe sepsis and obese BMI will have a decreased mortality risk in comparison with normal BMI patients.
Methods
The Trauma Quality Improvement Program (2017) was queried for adult trauma patients with documented BMI and severe sepsis. Patients were grouped based on BMI: non-obese trauma patients (nOTP) BMI <30 kg/m2 and obese trauma patients (OTP) ≥30 kg/m2. A multivariable logistic regression model was used for analysis of mortality.
Results
From 1246 trauma patients with severe sepsis, 566 (42.4%) were nOTP and 680 (57.6%) were OTP. OTP had increased length of stay (LOS) (19 vs 21 days, P < .001), intensive care unit (ICU) LOS (13 vs 18 days, P < .001) and ventilator days (10 vs 11 days, P < .001). After adjusting for covariates, when compared to normal BMI patients, patients who were overweight (OR 1.11 CI .875-1.41 P = .390), obese (OR .797 CI .59-1.06 P = .126), severely obese (OR .926 CI .63-1.36 P = .696) and morbidly obese (OR 1.448 CI 1.01-2.07 P = .04) all had a similar associated risk for mortality compared to patients with normal BMI.
Conclusion
In adult trauma patients with severe sepsis, this national analysis demonstrated OTP had increased LOS, ICU LOS, and ventilator days compared to nOTP. However, patients with increasing degrees of obesity had similar associated risk of mortality compared to trauma patients with severe sepsis and a normal BMI.
Keywords
Introduction
Obesity is a worldwide epidemic as it has nearly tripled since 1975. In 2016 the World Health Organization (WHO) reported that there were more than 1.9 billion adults over 18 years-old who were overweight, and of these 650 million were obese. Furthermore, the prevalence of obesity among the United States (U.S.) population was 36.9% between 2015-2016. 1 In addition, sepsis is one of the leading causes of death, with a prevalence of severe sepsis in the U.S of 300 cases per 100,000 population. 2 In fact, the Centers for Disease Control reported that as many as 6% of all reported deaths in the U.S. could be attributed to sepsis. 3 Thus, due to the high prevalence of obesity and sepsis, there is a need for studies which look at relationships between these highly morbid and lethal diseases.
One third of trauma patients have a prevalence of obesity.4,5 In a previous retrospective study done with 55,038 patients with sepsis Pepper et al found the mortality rate was inversely proportional to body mass index (BMI) 6 hence, obesity had a protective effect. However, other studies have found an increase in mortality, complications, length of stay, and ventilator days with obese trauma patients.7-10
Over 5 million adults between the years of 2012-2016 where discharge after a trauma with sepsis. 11 That said, there is a paucity of data on the effects of obesity regarding outcomes of trauma patients with severe sepsis. As such we sought to evaluate this relationship, hypothesizing that, trauma patients with severe sepsis and BMI ≥30 kg/m2 will have a decreased mortality risk in comparison with normal BMI patients.
Methods
After receiving approval from our Institutional Review Board (IRB), we performed a retrospective analysis of the Trauma Quality Improvement Program (TQIP). As this is a deidentified database no consent was required. We queried data from the year 2017 to identify all patients 18 years and older presenting to the hospital after trauma with an in-hospital complication of severe sepsis and documented BMI. Severe sepsis is a mandated reportable complication in TQIP and is defined by “sepsis plus organ dysfunction, hypotension (low blood pressure), or hypoperfusion (insufficient blood flow) to 1 or more organs.” We excluded all patients that died in the emergency department and patients with severe head trauma, defined by an abbreviated injury scale (AIS) grade for the head >3. Two groups were compared: non-obese trauma patients (nOTP) (BMI <30 kg/m2) and obese trauma patients (OTP) (≥30 kg/m2). The primary outcome was mortality.
Patient demographic information was collected including age, sex, lowest systolic blood pressure within 24 hours, and race. Information regarding comorbidities was also collected, including diabetes, hypertension, chronic obstructive pulmonary disease (COPD), and smoking status. Additional outcomes evaluated included total hospital length of stay (LOS), intensive care unit (ICU) LOS, and ventilator days. Complications were also evaluated including: acute renal failure, acute respiratory distress syndrome, cardiac arrest with cardiopulmonary resuscitation, decubitus, deep site infection, deep venous thrombosis, extremity compartment syndrome, myocardial infraction, organs space infection, pneumonia, pulmonary embolism, cerebrovascular accident, and urinary tract infection.
A Mann-Whitney-U test was used to compare continuous variables and chi-square was used to compare categorical variables. The data represented by categorical variables were reported by percentages while continuous data was represented with medians and interquartile range. Covariates were then controlled for using a multivariable stepwise-forward hierarchical logistic regression model. We compared increasing BMI groups: underweight (<18.5 kg/m2), overweight (25- 29.9 kg/m2), obese (30-35 kg/m2), severe obese (35-40 kg/m2), morbidly obese (≥40 kg/m2), to a reference group of normal BMI patients (18.5-25 kg/m2). After reviewing the literature and coming to a consensus among authors, we controlled for the following variables: age, alcohol use, hypertension, cardiac heart failure, diabetes mellitus, injury severe score, respiratory rate, pulse rate, systolic blood pressure, intensive care unit days, Glasgow coma scale.12-16
This was reported with an odds ratio (OR) and 95% confidence intervals (CI). All P-values were two-sided, with a statistical significance level of <.05. All statistical analyses were performed with IBM SPSS Statistics for Windows, Version 24. (Armonk, NY: IBM Corp).
Results
Demographics of Adult Trauma Patients With Severe Sepsis and Documented Weight
Demographics of Adult Trauma Patients with Severe Sepsis with Documented Weight.
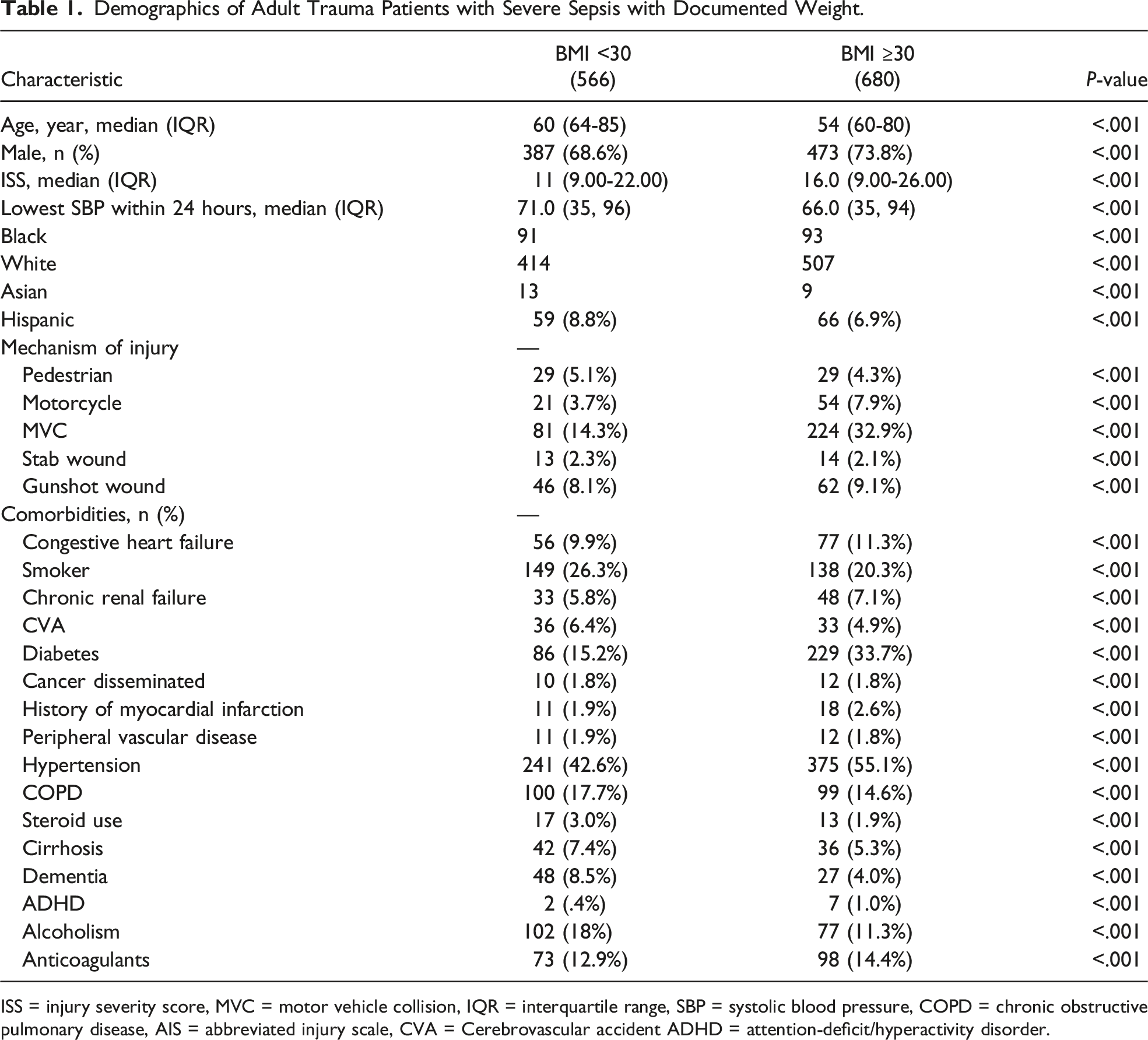
ISS = injury severity score, MVC = motor vehicle collision, IQR = interquartile range, SBP = systolic blood pressure, COPD = chronic obstructive pulmonary disease, AIS = abbreviated injury scale, CVA = Cerebrovascular accident ADHD = attention-deficit/hyperactivity disorder.
Clinical Outcomes of Trauma Patients With Severe Sepsis and Documented Weight
Clinical Outcomes of Trauma Patients with Severe Sepsis and Documented Weight.
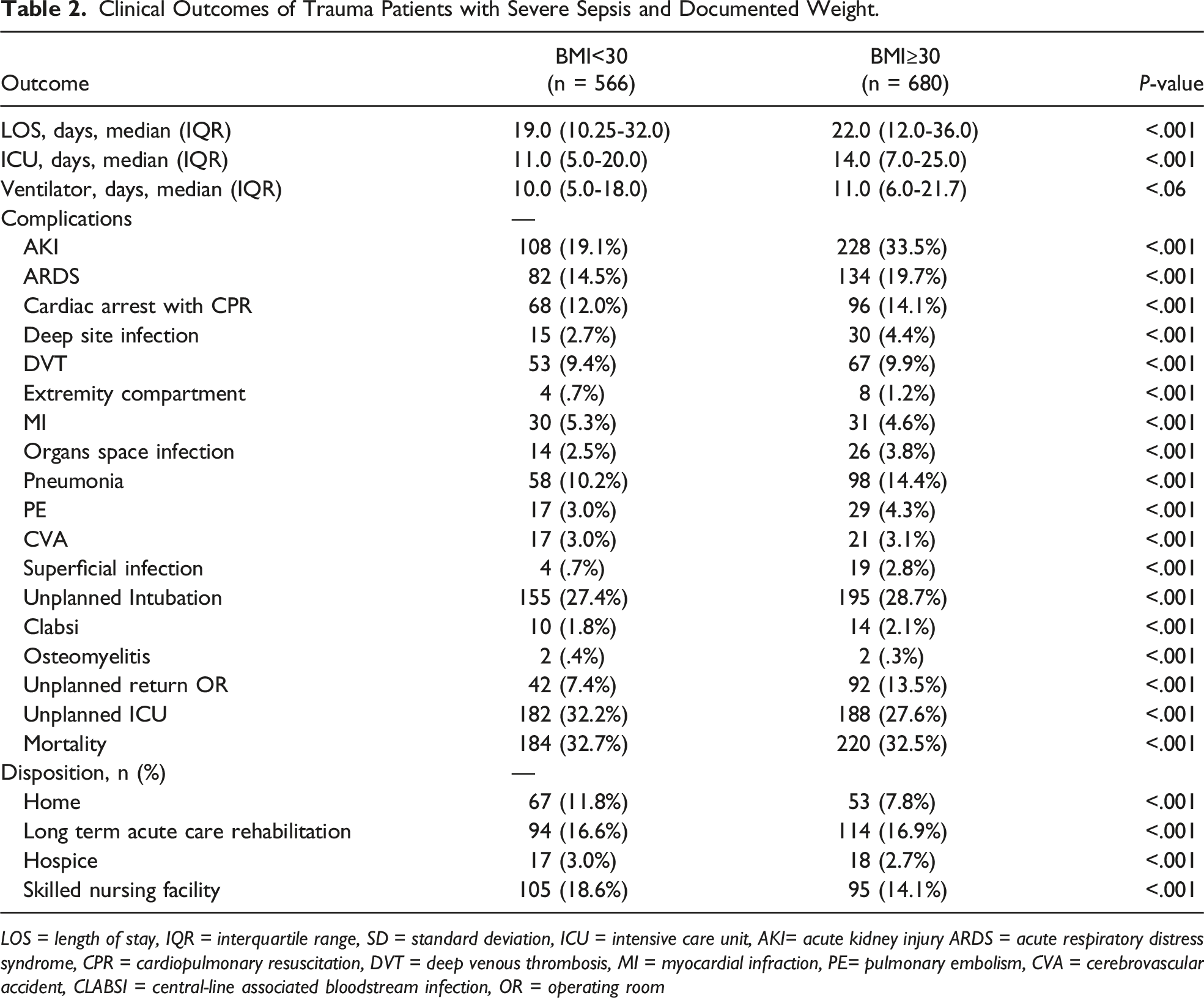
LOS = length of stay, IQR = interquartile range, SD = standard deviation, ICU = intensive care unit, AKI= acute kidney injury ARDS = acute respiratory distress syndrome, CPR = cardiopulmonary resuscitation, DVT = deep venous thrombosis, MI = myocardial infraction, PE= pulmonary embolism, CVA = cerebrovascular accident, CLABSI = central-line associated bloodstream infection, OR = operating room
Multivariable logistic regression analysis for risk of mortality in adult trauma patients with severe sepsis and different BMIs compared to patients with normal BMI.
Multivariable Logistic Regression Analysis For Risk Of Mortality In Adult Trauma Patients With Severe Sepsis With Different BMI Compared To Patients With Normal BMI.
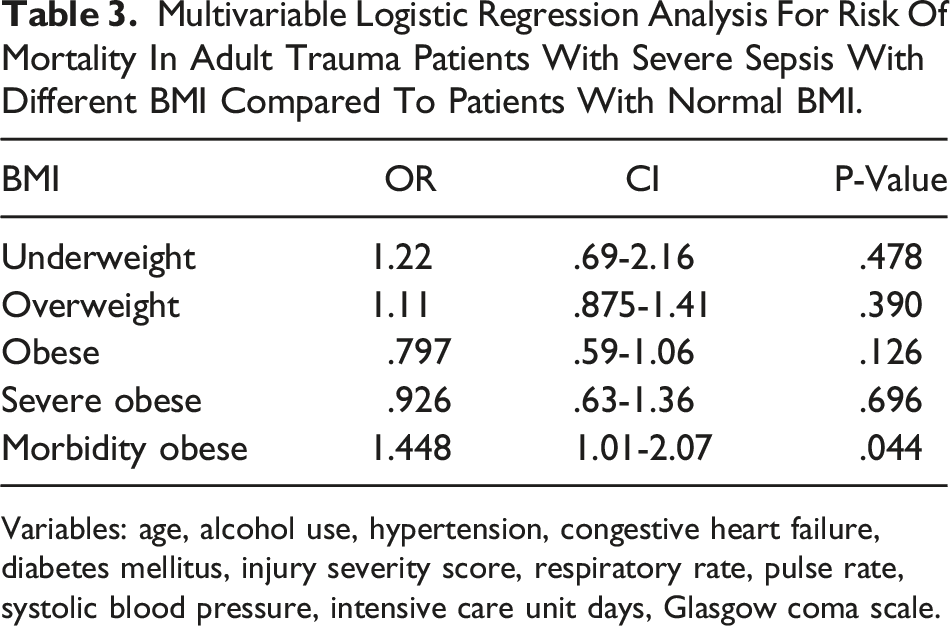
Variables: age, alcohol use, hypertension, congestive heart failure, diabetes mellitus, injury severity score, respiratory rate, pulse rate, systolic blood pressure, intensive care unit days, Glasgow coma scale.
A subset analysis of patients with ISS >15 was made. When compared with normal BMI patients, patient who were overweight (OR 1.08 CI .71-1.64 P = .699), obese (OR .629 CI .417-.95 P = .027), severe obese (OR .853 CI .519-1.403 P = .53), and morbidly obese (OR 2.396 CI 1.45-3.94 P = .001) all had a similar associated risk for mortality.
Discussion
This retrospective analysis using data from the TQIP database found an increased LOS, ICU LOS, and ventilator days in OTP in comparison with nOTP. In contrast, there was a similar rate and associated risk of mortality in OTP with severe sepsis and various BMI categories compared to normal BMI patients after adjusting for known predictors of mortality in trauma patients.
There is ongoing controversy regarding the impact that obesity has on severe sepsis and septic shock patients.6,17-21 Previously, Nguyen et al in a sample of over 1000 hospitals in the U.S. found that obesity was associated with a 16% decrease in mortality in patients with sepsis, however an increase of cost and LOS(18). Another retrospective study with 1,404 Medicare patients who were hospitalized with severe sepsis demonstrated an improvement in 1 year mortality with mortality rates of 44.7% in severely obese, 46.0% in obese, 53.1% in overweight, and 62.0% in normal weight patients (P < .001). 19 On the other hand, Gaulton et al in a retrospective cohort study of 1,779 adult non-surgical patients with sepsis found that obesity did not alter risk of mortality (1.11 95% CI .85-1.41. P = .47). 22 Our study, the first to our knowledge specifically evaluating OTP with severe sepsis similarly found no association with varying degrees of obesity with mortality. One possible explanation might be due to the source of infection in trauma patients differing from the predominantly medical patients seen in other studies. 23 Another possibility could be the fluid resuscitation that trauma patients receive differs from non-surgical patients, since trauma patients have been demonstrated to require significant fluid resuscitations due to concomitant injuries, it may be that these patients are more adequately resuscitated, which has been shown to improve outcomes.17,24-26 Alternatively, trauma patients have significant inflammatory pathways already activated, these factors may also overlap with the continuous activated inflammatory pathways that obesity already causes in the human body, thereby mitigating an effect that obesity has in non-trauma patients.3,27-30 Future prospective research, including basic science research regarding inflammatory pathways is needed to further evaluate our findings and ascertain why obesity may not have a protective effect in trauma patients with severe sepsis.
In addition, to the effect of obesity on mortality, prior studies have evaluated the effects of obesity on other outcomes such as LOS and ICU LOS. Arabi et al demonstrated an increased hospital LOS of approximately 3 days and ICU LOS for approximately 2 days in clinical patients with septic shock. 17 This is corroborated by multiple other studies on surgical and medical patients.17-19,31 Our study, unique to trauma patients, confirmed these findings demonstrating a 3 day increase in LOS and ventilator days and 5 days increase in ICU LOS for OTP. Thus, while our study demonstrated mortality does not change with varying BMIs, it does reveal an important difference in LOS. Given that hospitals are evaluated on outcomes including LOS these finding merits future evaluation and if confirmed than obesity should be incorporated into LOS metrics by TQIP and other benchmarking agencies.
As a retrospective database study there are many limitations to our study including those inherent to this study design, such as coding errors and missing data. Additional missing pertinent data variables within this database include: source and etiology and organism leading to severe sepsis, timing and classification of antibiotic therapies used, amount of fluid resuscitation given, procedures done in the ICU, and use of inotropic medications. Finally, TQIP is confined to index hospitalization, thus information regarding post-discharge outcomes and complications is unavailable. Therefore there is the need for prospective studies that can control for these variables and help understand better the influence of obesity in severe septic trauma patients.
Conclusion
In adult trauma patients with severe sepsis, this national analysis demonstrated that OTP had increased LOS, ICU LOS, and ventilator days compared to normal BMI patients. However, patients with increasing degrees of obesity had a similar associated risk of mortality compared to trauma patients with severe sepsis and a normal BMI. Prospective validation of these findings is necessary to definitively clarify the role of obesity in severe sepsis trauma patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.