
Abstract
Background:
Cardiovascular morbidities like arterial stiffness and atherosclerosis have a negative association with insulin resistance, which can be identified by carotid intima media thickness (CIMT) measurement. One-hour postload plasma glucose (1 h-PPG) is a novel marker for early identification of insulin resistance, but very few studies are available on its relationship with CIMT.
Objective:
To identify the correlation of CIMT with 1 h-PPG in overweight and obese adults without diabetes.
Methods:
Individuals not having known diabetes or other chronic illnesses were identified and subjected to the initial anthropometric analysis for body mass index (BMI) calculation. A standard oral glucose tolerance test was performed on individuals with a BMI of ≥25 kg/m2 for 1 h-PPG values, and a B-mode ultrasound scan of the neck was used for CIMT measurement. A Pearson’s correlation statistical test was applied for correlation identification.
Results:
A total of 94 nondiabetic individuals participated, of whom 55 (58.5%) were women. Mean age, BMI, and CIMT values of the study population were 38.8 (±8.09) years, 29.6 (±3.22) kg/m2, and 0.72 (±0.10) mm, respectively. Average 1 h-PPG levels were 150.7 (±21.11) mg/dl, and the Pearson’s coefficient (r) value with CIMT was 0.5792 (P < 0.05). Further, correlation analysis demonstrated an r-value of −0.0029 for BMI, −0.1293 for waist-hip ratio, −0.0047 for waist-height ratio, 0.3862 for glycated hemoglobin (HbA1c), and −0.2930 for 2 h-PPG.
Conclusion:
In euglycemic adults, the early insulin resistance defining parameter, i.e., 1 h-PPG levels had a consistent positive correlation with CIMT, which is a marker of the initial stages of atherosclerosis.
Keywords
INTRODUCTION
Insulin resistance is a rapidly growing public concern, leading to numerous health hazards and target organ damage. The infirmity has a consistent relationship with atherosclerosis and other adverse cardio-vascular (CV) events, and early postmeal hyperglycemia is the first sign of insulin resistance development. A report by Sciacqua et al. demonstrated that in intermediately hyperglycemic subjects, arterial wall stiffness (a surrogate endpoint for CV disease), and aortic hemodynamic parameters are significantly higher when compared to nonhyperglycemic subjects.[1] Another study on 644 diabetics found that the maximal increase in blood glucose 1 h postmeal has a stronger association with carotid arterial wall thickness than other markers of glycemic control such as HbA1c, fasting plasma glucose (FPG), and two-hour postmeal plasma glucose (2 h-PPG).[2] Further, raised plasma glucose levels have been firmly associated with diabetic cardiomyopathy in a recent work.[3] The literature has also documented that the HbA1c level, which is a reflection of chronic hyperglycemia, has a direct correlation with ischemic cardiac events, even at levels below the diagnostic cut-off for overt diabetes.[4] These findings point to intermediate hyperglycemia as a possible cause of vascular anatomy changes. For early identification of this hyperglycemia or insulin resistance, various tools have been studied, and one such novel parameter is one-hour postprandial plasma glucose (1 h-PPG).
Atherosclerosis is an early and crucial step in the development of macrovascular complications, including the CV system. Examination of the carotid artery vessel wall provides an opportunity to assess subclinical variations within the wall structure or atherosclerosis that anticipate and predict the future development of CV clinical events. To predict these outcomes and early atherosclerosis, carotid intima media thickness (CIMT) measurement by ultrasound (USG) scan has been recommended by the American Society of Echocardiography.[5] Raised CIMT values have been associated with a higher incidence of coronary heart disease and stroke, even in asymptomatic individuals.[6] A recent study from India looked at CIMT in diabetic patients and discovered increased carotid intima thickness as well as a positive correlation with FPG and 2 h-PPG.[7] However, the correlation of CIMT with 1 h-PPG and its comparison with other obesity and dysglycemia defining parameters have been rarely described in the current literature. Also, various studies have documented that nondiabetic individuals or people with traditional diabetic markers below diagnostic cut-offs, are also prone to CV complications like arterial stiffness and atherosclerosis, but there are very few studies dealing with this issue.[4,8] Thus, in this research, the correlation of CIMT with 1 h-PPG was studied to identify early CV morbidity in overweight and obese nondiabetic north Indian adults.
Objective of the study
To identify the correlation of CIMT with 1 h-PPG in overweight and obese adults without diabetes.
METHODS
Design and study population
In this observational study, apparently healthy North-Indian adults of age 18–50 years were identified over the course of 1 year (January 2019-December 2019). After explaining the study protocol, individuals underwent anthropometric measurements for body mass index (BMI), waist-hip ratio (WHR), and waist-height ratio (WHtR) calculations. Persons with known diabetes and chronic diseases like chronic liver disease, chronic kidney disease, thyroid disorders, and chronic pancreatitis were not included. Long-term substance abusers, smokers, and individuals on chronic medications like statins, steroids, beta blockers, and thiazides were also excluded.
Laboratory and oral glucose tolerance test evaluation
Individuals with a BMI of ≥25 kg/m2 (as per the WHO BMI cutoff for identification of overweight and obese subjects) underwent additional biochemical tests, which included a complete blood count, a renal function test, hepatic enzymes, a lipid profile, and HbA1c levels. Also, a standard 75-gm oral glucose tolerance test (OGTT) as per the WHO protocol was conducted after a fasting period of 8 h–12 h, and blood samples were collected for FPG, 1 h-PPG, and 2 h-PPG values.[9]
Carotid intima media thickness measurement
The CIMT measurement was done by an experienced radiologist. For the measurement, the individual lied in a supine position with their neck extended and the head rotated 45° toward the side opposite to the side being imaged. Scanning was performed with a high resolution B-mode USG scanner (Philips® IU 22 Unit), using a linear transducer of 7–17 MHz frequency. The thickness was measured separately at the midpoint of the common carotid artery (far wall of the common carotid artery) on both sides, using minimal compression on the artery. Automated measurements of CIMT were done in a 10 mm segment of the artery.
Statistical analysis
All necessary measurement data were entered into Microsoft Excel® 2016 for further calculation. Results related to continuous data were expressed as mean and standard deviation (±SD). Anthropometric and laboratory characteristics of all the participants were compared using the t-test. Similarly, for the objectification of the relationship between CIMT and 1 h-PPG, and other parameters like BMI, WHR, WHtR, HbA1c, and 2 h-PPG, Pearson’s correlation analysis was performed. The mean value of CIMT, after adding both the right and left values, was used for relationship analysis. A P < 0.05 was considered significant.
Ethical approval and consent to participate
This study was approved by the ethics committee of the Government Medical College and Hospital, Chandigarh, with letter no. GMC/IEC/2018/167. Written consent was obtained from each of the study participants, and the basic principles of respect for autonomy (including truth-telling, informed consent, and confidentiality), beneficence, nonmaleficence, and justice were adhered to at all times.
RESULTS
Description of study population and anthropometric result
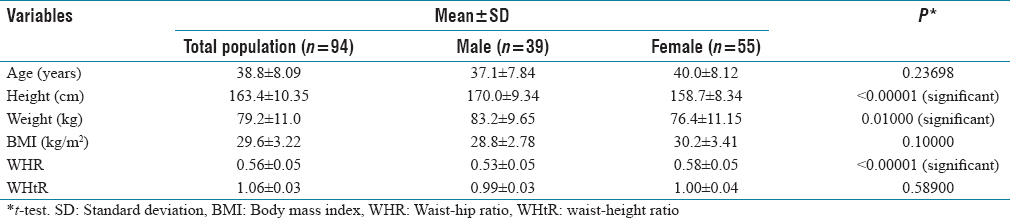
A total of 98 overweight and obese individuals were enrolled, but 4 were excluded due to FPG, 2 h-PPG, and HbA1c levels above the diagnostic cut-off for diabetes. The study population consisted of 94 euglycemic adults (55 females and 39 males). The mean age of the study population was 38.8 (±8.09) years, and the average BMI was 29.6 (±3.22) kg/m2. Females had a higher BMI (30.2 kg/m2) and WHtR but a lower WHR than the total population [Table 1].
Anthropometric characteristics of the study population
Basic laboratory investigations depicted that mean total cholesterol levels were slightly different in both groups, but the average triglyceride levels were significantly raised among males (227.4 vs. 197.2 mg/dl) [Table 2]. Both groups had nearly identical high density lipoprotein levels (38.5 and 39.7 mg/dl), but more unfavourable for the female group as per the desired cut-off. HbA1c levels were 5.74% among female participants and 5.48% among males, with a significant P value (<0.05). Likewise, 1 h-PPG and 2 h-PPG average levels were higher in females. This demonstrates an elevated dysglycemic condition in the overweight and obese female population. The average value of CIMT for the total population (0.72 mm) was similar to that for the female population (0.72 mm) and higher than the male population (0.71 mm).
Laboratory characteristics of the study population

Correlation of HbA1c, 1 h-PPG, 2 h-PPG with carotid intima media thickness
The correlation analysis between 1-h post-OGTT plasma glucose and CIMT found a positive r = 0.5792, with a statistically significant P value (<0.05) [Figure 1]. CIMT also had a positive but weaker Pearson’s coefficient value with HbA1c (0.3862, P < 0.05). Furthermore, the evaluation described a statistically significant negative correlation association between CIMT and 2 h-PPG [Table 3] among overweight and obese study individuals.

Scatter plot demonstrating correlation between 1 h-PPG and carotid intima media thickness values
Correlation between carotid intima-media thickness and different study parameters

Correlation of body mass index, waist-hip ratio and waist-height ratio with carotid intima media thickness
The Pearson’s coefficient (r-value) between BMI and CIMT was −0.0029, with an insignificant P value. Also, the correlation calculation expressed an r value of −0.1293 for WHR (P > 0.05), and −0.0047 for the WHtR and CIMT association (P > 0.05) [Table 3].
DISCUSSION
In the present study, 94 nondiabetic overweight and obese adults were evaluated for the association of CIMT with different insulin resistance and obesity defining parameters. The female population predominated among the participants. This is consistent with previously collected data from this geographical region demonstrating a higher prevalence of obesity and insulin resistance in females.[10] However, Youn et al. and Eric et al. observed higher CIMT values in the male population despite exhibiting similar obesity indices among both genders.[11,12] The average BMI of the present study population fell in the overweight category, which is an initial move toward morbid obesity, and identification of this point is crucial in terms of halting adverse events.[12]
Insulin resistance or hyperglycemic denoting elements like HbA1c, 1 h-PPG, and 2 h-PPG levels, were also assessed for correlation with CIMT, and among these, 1 h-PPG had a strong association with carotid thickness. Although less strongly than 1 h-PPG, HbA1c levels showed a positive correlation, while 2 h-PPG levels showed a negative association. As HbA1c defines chronically elevated plasma glucose levels, Choi et al. demonstrated its positive association with peripheral arterial disease.[13] But the same research failed to identify any association between HbA1c and CIMT, even in the presence of T2DM. However, comparable to another community-based investigation on 1627 participants, our HbA1c result depicted a statistically significant positive correlation with CIMT.[14] This study by Huang et al.[14] also described a significant association between HbA1c and CIMT in normal glucose tolerant individuals that was independent of FPG and 2 h-PPG values.
In this research on overweight and obese adults, 1 h-PPG values correlated more positively with CIMT than any other parameter and had a significant association (P < 0.05). The importance of this intermediate hyperglycemia in the context of raised CIMT values was also depicted in research by Esposito et al. that included T2DM subjects for the correlation assessment.[2] The result demonstrated a positive association in already diagnosed individuals with T2DM, and our study followed this association, even in euglycemic subjects. Esposito et al. study also demonstrated that after a meal, plasma glucose level achieves peak at 1-h postfood intake. In an analysis by Temelkova-Kurktschiev et al., OGTT was performed among 582 individuals without known diabetes history, and correlated 30, 60, 90 and 120 min PG with CIMT.[15] This study found that OGTT-based variables, including 1 h-PPG, were significantly associated with CIMT, except for 30 min postload PG, and FPG levels. The combined results of these studies and our observations depict a plausible correlation of 1 h-PPG with CIMT. Additionally, raised plasma glucose affecting the vascular endothelium and altering the normal intimal physiology is also proven at the molecular level by various studies.[16,17]
A recent literature found that individuals with uncontrolled diabetes had thicker CIMT than their nondiabetic and well controlled diabetic counterparts, but there was no correlation between 2 h-PPG and CIMT values, similar to our observation.[18] These findings suggest the superior nature of intermediate hyperglycemia in diagnosing early atherosclerosis. Furthermore, Tenjin et al. concluded the plasticity behaviour of CIMT, and the observed values of CIMT in this study improved after hyperglycemia treatment.[19] Thus, hyperglycemia, especially deranged 1 h-PPG levels, has a significant association with raised CIMT values, and measurement of this pathological abnormality can identify a major risk factor for an adverse CV profile. The negative impact of 1 h-PPG is not limited to vascular thickness alteration, but various other harmful ailments have been demonstrated. In a study on South Indian adults with an 11-year follow-up, it was observed that individuals with elevated 1 h-PPG levels had more tendencies for the development of diabetes mellitus.[20] Also, progression to diabetes mellitus was also higher in Indians with deranged 1 h-PPG values, as observed by Priya et al. in 1179 subjects.[21] In another study by Paddock et al., 1 h-PPG levels were found to be equally effective in diagnosing diabetic retinopathy.[22]
The comparison of obesity defining parameters, i.e., BMI, WHR, and WHtR with CIMT demonstrated that these parameters had a weak association with atherosclerotic arterial changes in overweight and obese individuals. Ge et al.’s recent study on BMI and CIMT on 526 people found no link between BMI and CIMT.[23] Moreover, Eric et al. observed a weakly positive but statistically insignificant association between these two parameters.[12] Our observations are similar to these studies, nullifying the effect of BMI on CIMT. Likewise, for WHR and WHtR, CIMT had a negative coefficient (r value). Equivalent results were expressed by a previous study on 4216 Brazilian adults, which concluded that WHtR has no association with CIMT.[24]
One important strength of this study was the concomitant evaluation of both obesity and insulin resistance defining parameters in euglycemic North Indian population, and the results obtained in this research are more feasible for comparison among these parameters. The limitations of this study include a relatively small sample size and single-centre participant inclusion. Another limiting factor can be the use of USG scan for CIMT measurement, which can have observer based variations, but to avoid this, the scan was performed by a single, highly experienced radiologist. Also, the modality is readily available, noninvasive, and less time consuming, so it can be used in resource limited settings. A deranged lipid profile could be a confounder for thick CIMT, but all the parameters were assessed in the same population, and only two parameters had significant associations with CIMT (i.e., Hb1Ac and 1 h-PPG).
In recommendation, application of 1 h-PPG post-OGTT in high risk individual is time saving and more reliable than 2 h-PPG measurement, and may act as a better surrogate marker of a poor cardio-metablic profile. Thus, a 1 h-PPG measurement during OGTT could be additionally considered for risk stratification in addition to the traditional markers.
CONCLUSION
In this study, early atherosclerosis defining marker, i.e., CIMT, had a positive and significant correlation with 1 h-PPG, which defines that intermediate hyperglycemia may exhibit an adverse CV profile among nondiabetic overweight and obese individuals. The research also concluded that obesity defining tools like BMI, WHR, and WHtR were relatively inferior in this context, HbA1c had a relatively weak correlation, and 2 h-PPG levels had no association with CIMT.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
The study was ethically approved from institutional ethics committee/institutional review board with letter no. GMC/IEC/2018/167.
Consent to participate
The participants, who gave positive written informed consent after explaining the study and objectives, were included in this study. None of the study participant was exposed to any invasive procedure and all of the participants were assured that confidentiality of their personal data would be maintained.
Funding
Nil.
Author contribution
All of the authors contributed to the study conception and design. The idea for the article was conceived by MG and GJ. Material preparation, data acquisition, data collection and analysis were performed by GJ, MG, NK and SG. The first draft of the manuscript was written by GJ and MG and all authors commented on versions of the manuscript. GJ and MG performed the literature search and data analysis, while NK and SG critically revised the work. All authors read and approved the final manuscript.