
Abstract
Obesity is a chronic relapsing disease with rising prevalence in South Asia because of the changing economic and social landscape and transition in lifestyle. The issues in obesity management are unique to South Asians because of the characteristic ‘thin-fat’ phenotype, diet with high carbohydrate and low protein contents, issues with availability, affordability and approval status of various anti-obesity drugs and various social and cultural aspects unique to this population. In this article, we have reviewed literature sourced from India and South Asia pertaining to obesity and addressed the steps for a comprehensive and streamlined approach for the management of obesity in this part of the world.
Keywords
Obesity is a chronic disease with a high potential for relapse. In order to emphasise this fact, the term ‘Adiposity Based Chronic Disease’ (ABCD)[1] was coined by the American Association of Clinical Endocrinology (AACE) to refer to obesity. There is a tremendous rise in prevalence of obesity in South Asia in the recent decades, and various factors contribute to it, like rapid rate of urbanisation, sedentary lifestyle and change in food habits especially among the younger population. According to the World Obesity Atlas 2024, the global estimate of people with BMI ≥ 25 kg/m2 was 2.2 billion in 2020, of which 335 million were from the South East Asia region. This burden is projected to increase to 3.3 billion worldwide in 2035, out of which 607.57 million will be from the South East Asia region only. Looking at the data available from 2000 to 2016, all the South Asian countries are among the top 20 countries worldwide for the most rapid increase in the proportion of adults living with high BMI.[2] The diagnosis and management of obesity should be curated for the South Asian context. This review enumerates the unique challenges in diagnosis and management of obesity in South Asia.
Parameters Indicating Obesity
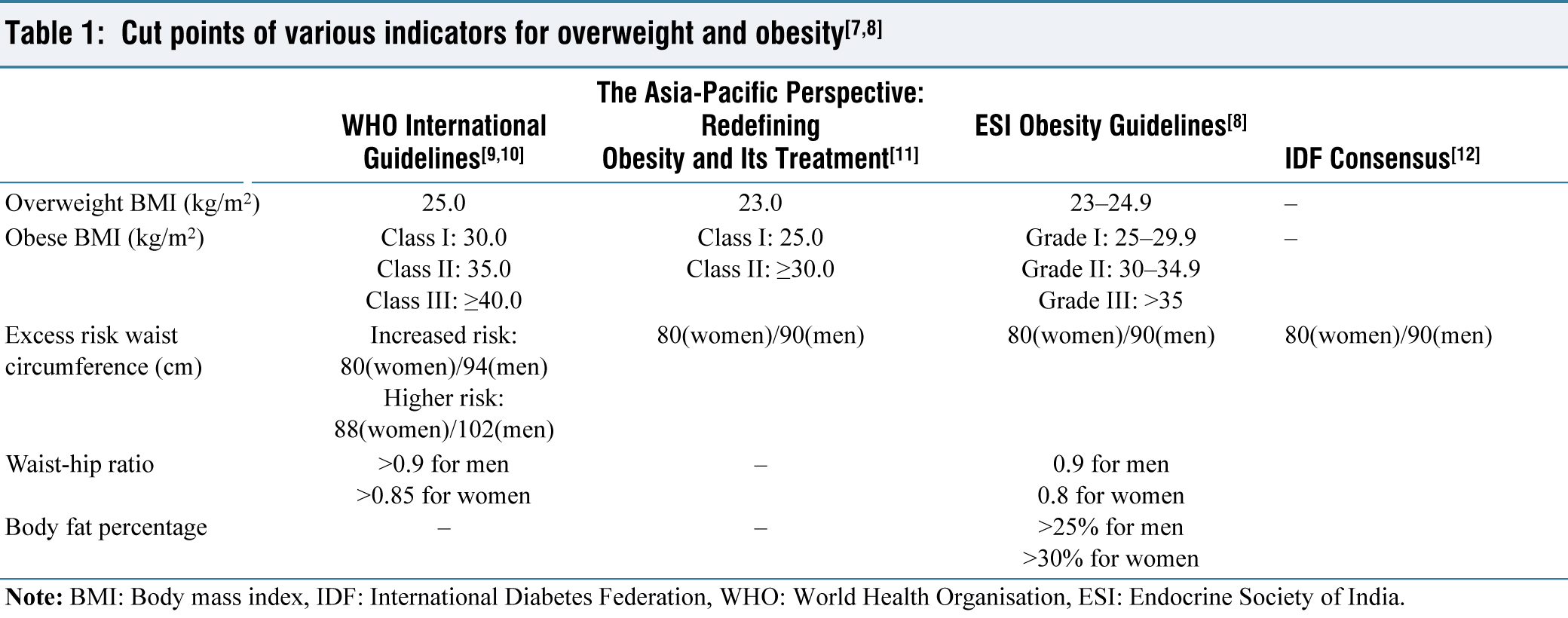
The BMI cutoffs for defining overweight and obesity are lower in the Asian population as compared to international cutoffs due to the concept of thin fat phenotype with higher visceral fat for the same BMI in South Asians as compared to the Caucasian population [Table 1].[3] South Asians have higher insulin resistance and cardiometabolic risk at lower BMIs.[4-6]
Assessment of Patients with Obesity
As obesity is a multifaceted chronic disease with multiple complications and associated comorbidities, the evaluation for the same should be broad enough to address to all such aspects. Numerous guidelines have stressed the significance of employing detailed clinical staging systems like the Edmonton Obesity Staging System (EOSS) alongside evaluating the aetiology of obesity and assessing associated comorbidities.
The EOSS is a comprehensive clinical staging system which takes into account the risk factors related to obesity, physical and psychological symptoms and functional limitations for disease staging.[13] This staging system not only helps in predicting mortality but also in designing a plan for the treatment of obesity as well. People with obesity (PwO) who have BMI >23 kg/m2 or WC > 80 cm for women and >90 cm for men should undergo the EOSS staging system for staging and planning therapeutic interventions.[14]
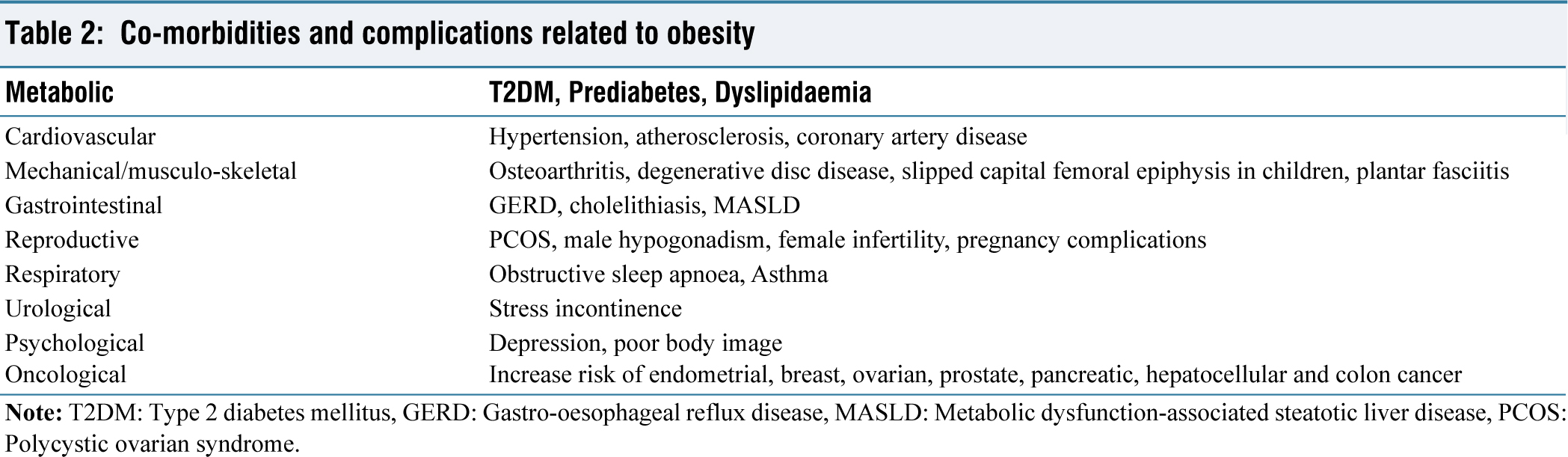
A comprehensive comorbidity and complications assessment should be done in PwO [Table 2].
Co-morbidities and complications related to obesity
Treatment of Obesity
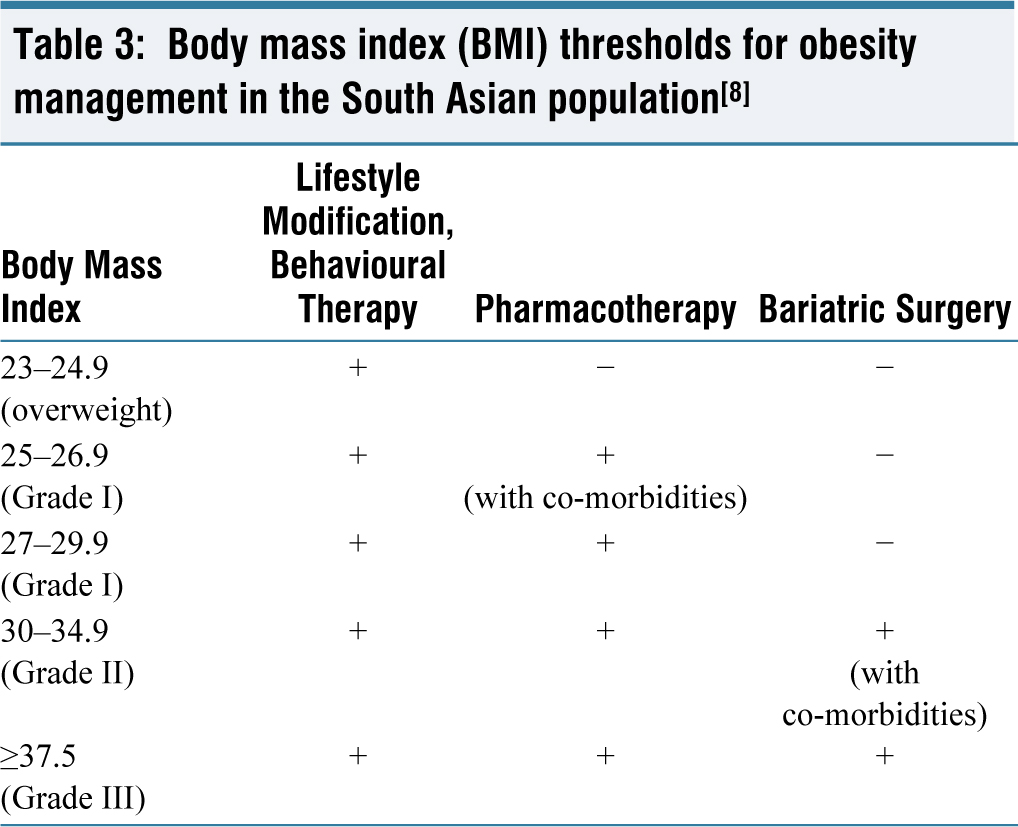
The goals of obesity management should be aimed at prevention of further weight gain, reducing weight and maintenance of the lower body weight achieved. Along with weight loss, treatment should be targeted to improving metabolic health, developing a positive body image, addressing comorbidities and overall, well-being. Achieving a weight loss of 5%-10% within six months is a practical target and offers several metabolic benefits [Table 3].[15]
Body mass index (BMI) thresholds for obesity management in the South Asian population[8]
Lifestyle Modification
Lifestyle modification combines dietary modifications, physical activity and behavioural therapy. It is the first rung in the ladder of obesity management.
Diet in Obesity
In planning a diet for obesity, the goal should be to lower overall calorie intake while maintaining adequate nutritional value. The patient’s cultural culinary habits, personal choices, affordability, compatibility with other co-morbidities and potential to continue over a prolonged time period need to be considered while designing a diet plan. The patient needs to be educated about unhealthy foods and food habits. A food diary or journal would be useful to track daily meals, and hence avoid eating at irregular intervals, frequent snacking or skipping meals.
The dietary modification with calorie restriction, modification of macronutrient composition and portion control are required for a long-term effective weight loss. South Asian population have a characteristic macronutrient distribution with high carbohydrate and low protein content compared to the western diet. This is responsible for the typical thin fat Indian phenotype with sarcopenic obesity.[8]
Calorie restriction can be started by restricting >500 kcal per day, targeting 0.5 kg-1 kg of weight loss per week or 8%-10% weight loss over six months’ time.
Physical Exercise
Studies have shown that South Asian people are physically less active[16,17] compared to the western population and also their participation in recreational activities is uncommon, especially among women and elderly[18,19] which in turn contributes to the increased prevalence of obesity in this subset of population. Regular physical exercise not only helps in weight loss but also has other benefits like improvement in cardiometabolic risk factors, improvement in body image, mood disorders and reduction of dementia and cognitive decline.[20-23]
Aerobic exercise of moderate intensity of ≥150 min/week done in three to five daily sessions per week not only helps in modest weight loss, but also in reducing visceral fat[24] and in maintenance of weight after weight loss.[25] Resistance training is recommended two to three times a week in patients undergoing weight loss therapy, which includes single-set exercises that involve major muscle groups, as it helps promote weight loss and maintain fat-free muscle mass.[26-29] Escalating to 300 minutes a week of moderate-intensity, or 150 minutes a week of vigorous-intensity aerobic physical activity can have probable benefit given the dose response relationship between physical activity and health.
However, while prescribing an exercise regimen for any patient, his/her age, physical status, disability, co-morbidities and motivation to adhere to the regimen must be considered. It is recommended that patients with co-morbidities undergo a pre-participation medical consultation before starting an exercise regimen.
Pharmacotherapy in Obesity
Pharmacotherapy is recommended for individuals with a BMI greater than 27 kg/m² or for those with a BMI over 25 kg/m² who have one or more associated comorbidities like Type 2 diabetes, hypertension, dyslipidaemia, obstructive sleep apnoea, etc. or at lower BMIs for individuals who are unable to exercise.
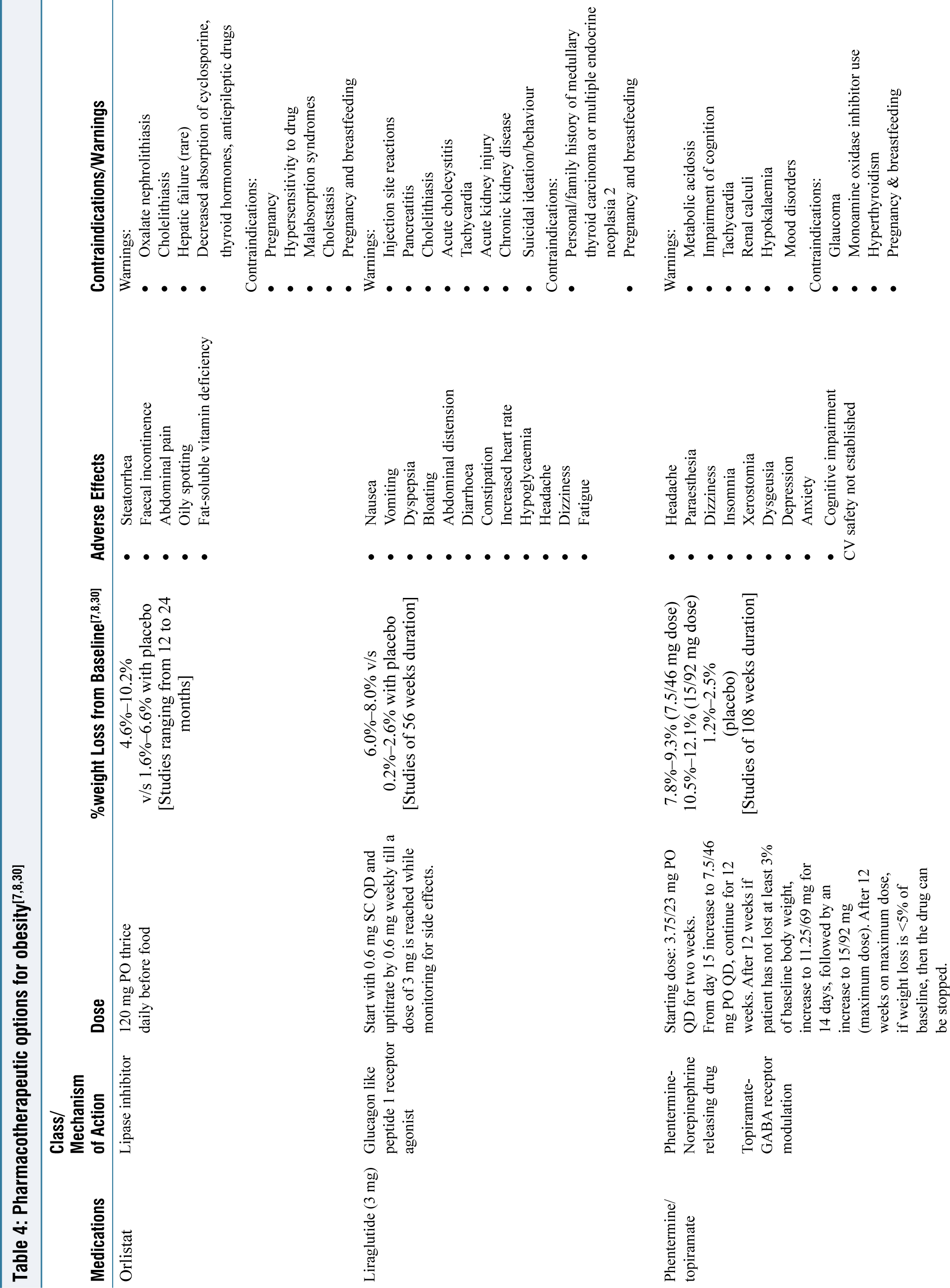
The most commonly used drugs in South Asia for obesity are orlistat, liraglutide and phentermine. However, Orlistat is the only approved drug for pharmacotherapy of obesity in India.
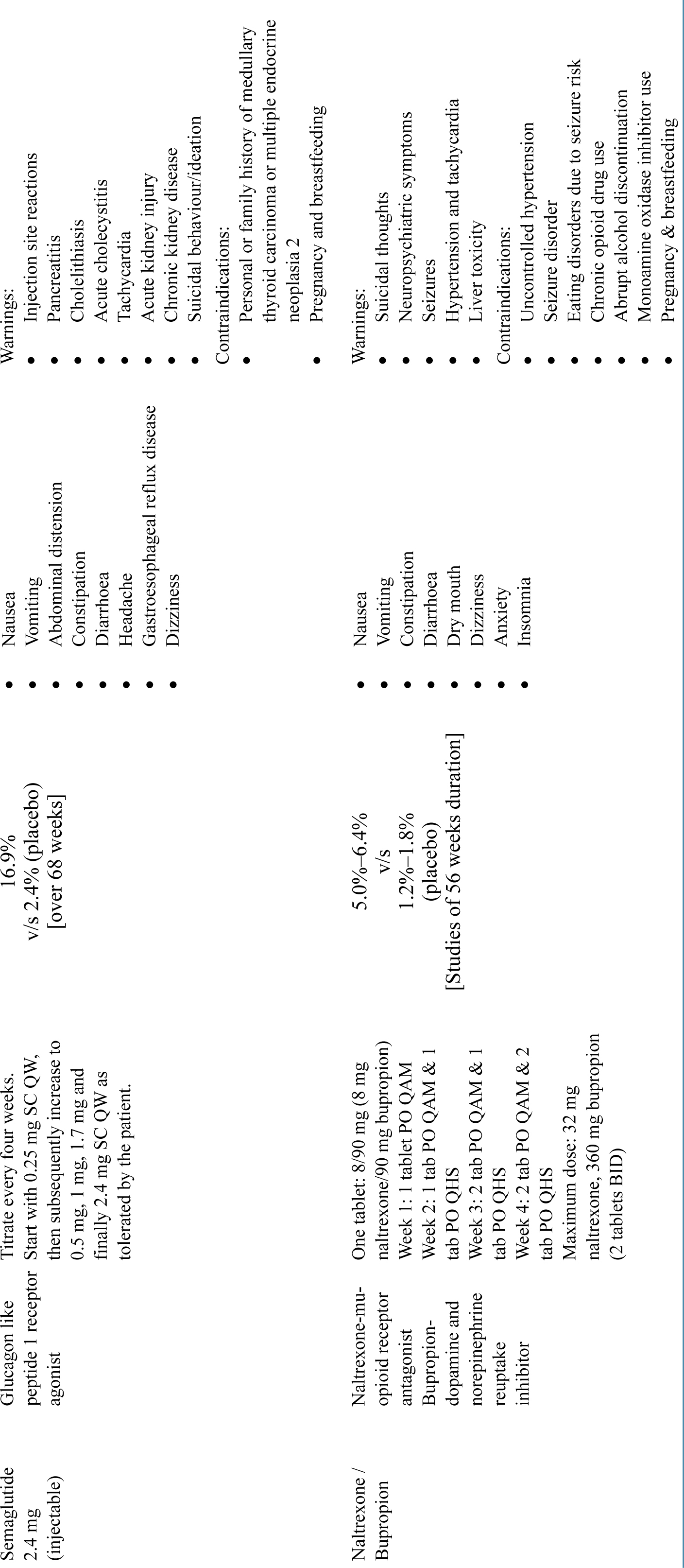
After starting the drug, it is advisable that the patients are monitored once monthly for three months, followed by once in three months thereafter. A drug is considered ineffective and can be discontinued if it fails in reducing the body weight by 5% in adults.[30] It should be kept in mind that pharmacotherapy should always be used as an adjunct to lifestyle modification and never alone. Short term pharmacotherapy has not proven to reduce long term complications of obesity and there is often weight regain when the drug is stopped [Table 4].[31-33]
Newer Drugs
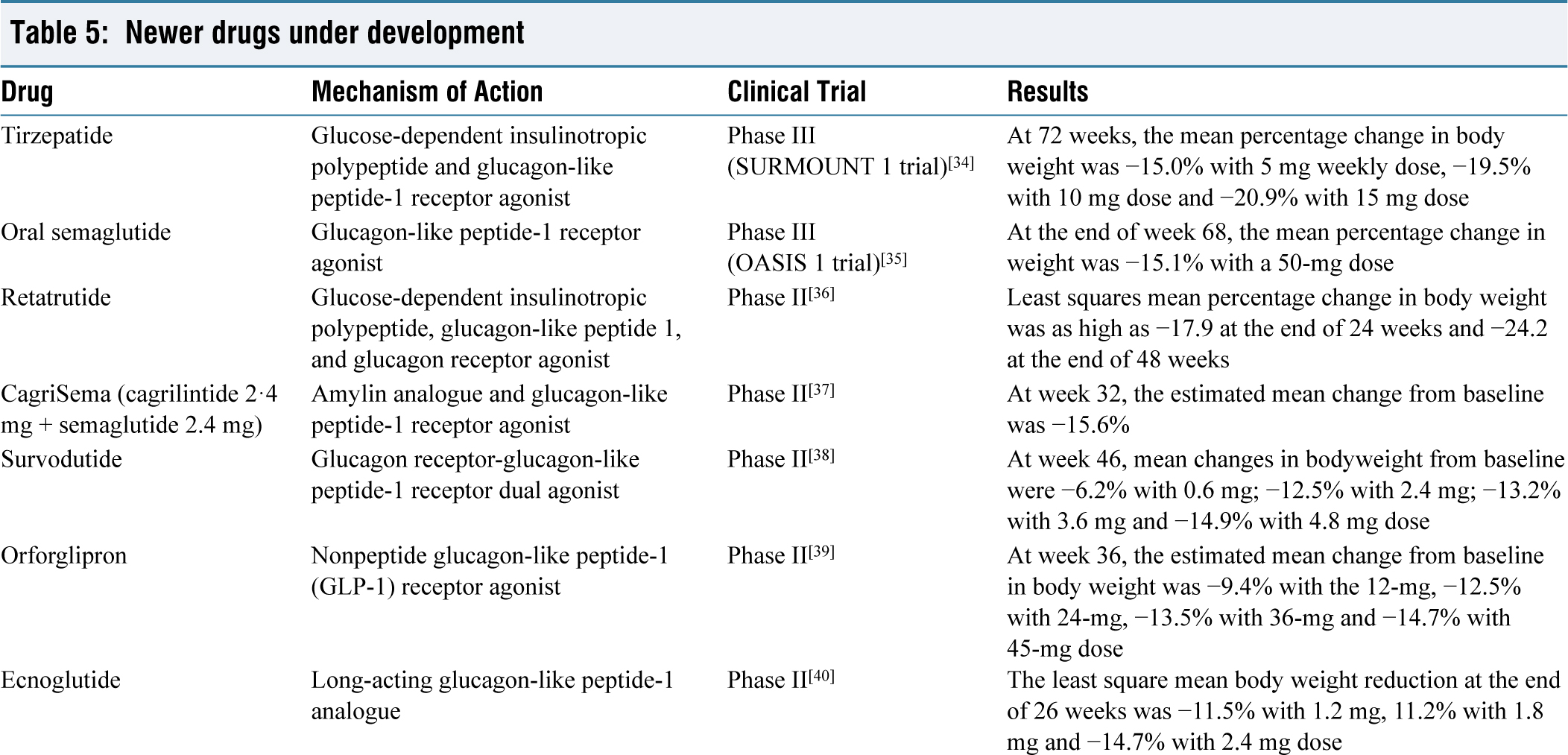
Several newer molecules have shown promising results for obesity management in phase 2 and phase 3 trials, which are going to be available in the market in the near future [Table 5].
Newer drugs under development
Certain drugs have been approved for use in monogenic/syndromic obesity like setmelanotide and metreleptin.
Setmelanotide, a melanocortin 4 receptor (MC4R) agonist, is FDA-approved for treating obesity in adults and children over six years old caused by deficiencies in proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1) or leptin receptor (LEPR). It has also received supplemental indication for obesity associated with Bardet-Biedl Syndrome.
A leptin analogue, metreleptin has been approved for management of obesity and other complications of leptin deficiency in patients with congenital or acquired generalised lipodystrophy.
Bariatric Surgery
Bariatric surgery predominantly involves three kinds of procedures: restrictive procedures, malabsorptive procedures and combined procedures. Restrictive procedures involve reducing the gastric volume and increasing satiety with smaller portions of food. Malabsorptive procedures include changing the path of the gastrointestinal tract via resections and anastomoses to cause malabsorption and combined procedures involve elements of both.
Restrictive procedures: Laparoscopic adjustable gastric banding, vertical sleeve gastrectomy, vertical band gastroplasty and intragastric balloon.
Malabsorptive procedures: Jejuno-ileal bypass, bilio-pancreatic diversion with duodenal switch.
Combined procedures: Roux-en-Y Gastric Bypass (RYGBP)
The indications for bariatric surgery according to western guidelines are BMI ≥ 40 kg/m2 or BMI ≥ 35 kg/m2 with at least one obesity related complication/comorbidity. For South Asians, indications for surgery are as mentioned in Table 6.
Indications for bariatric surgery
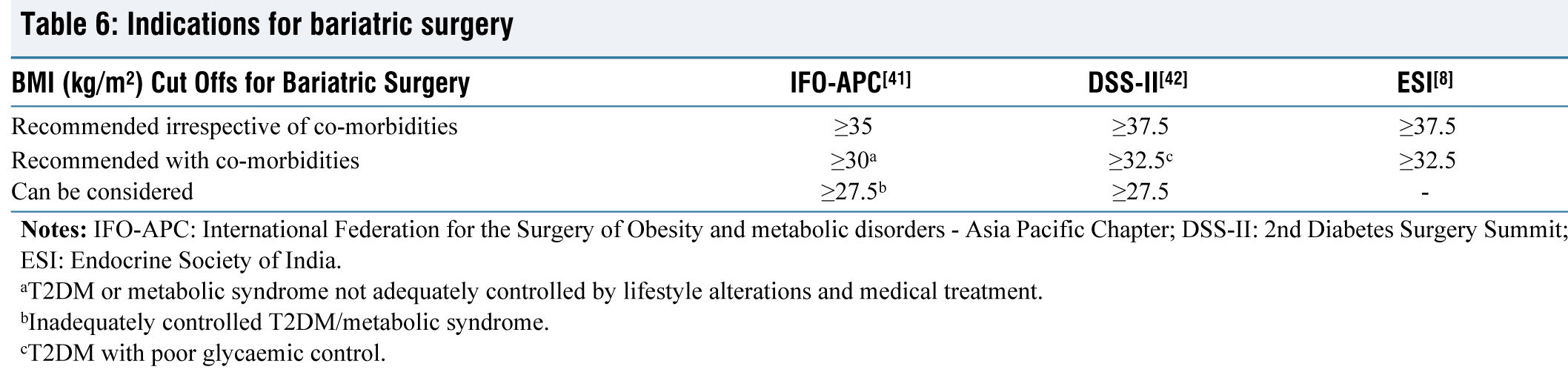
aT2DM or metabolic syndrome not adequately controlled by lifestyle alterations and medical treatment.
bInadequately controlled T2DM/metabolic syndrome.
cT2DM with poor glycaemic control.
The amount of weight loss after bariatric surgery depends on the type of surgery done. Gastric bypass, gastric band and sleeve gastrectomy lead to loss of 14–20, 8–12 and 10–18 units of BMI respectively.[43,44] Apart from weight loss, studies have also shown remission of T2DM[45,46] and improvement in dyslipidaemia and decrease in systolic blood pressure with bariatric surgery.[47,48] However, surgery may not be suitable for all populations and is contraindicated in patients with reduced life expectancy, substance abuse, untreated schizophrenia and a history of non-adherence to previous medical care. Post surgery patients may require permanent dietary modifications or micronutrient supplementation and should be counselled before surgery about such consequences.
Follow-up and Maintenance of Weight Loss
As mentioned earlier, obesity is a chronic relapsing illness and despite initial weight loss, regain of weight is common and patients need to be educated regarding this fact. It is important to give realistic targets and expectations in order to prevent disappointment and loss of motivation to adhere to lifestyle modifications and treatment. While designing a dietary plan or exercise regimen for a patient, care should be taken that it is done in such a way that the patient has maximum adherence to the prescribed treatment regimens. Follow up visits to be scheduled at least every three months. A multidisciplinary team should be involved in the follow-up care of the patient, which addresses different domains like diet, exercise, pharmacotherapy and psychological support. At each visit, weight measurement to be done and investigations as needed for co-morbidities/for assessing metabolic health. Caregivers should emphasise adherence to diet and exercise at every visit and educate the patients on pharmacotherapy that medications are used as an adjunct to lifestyle modifications and not alone.
Current Concepts in Obesity Definition
Most guidelines rely on excess adiposity alone, mostly measured by BMI in defining obesity as a disease. However, there are several limitations to this approach:
Preserved health can exist in the face of increased adiposity. BMI alone does not provide any information on the health of the individual. BMI can underestimate (e.g., elderly, South Asians, etc.) or overestimate (e.g., Athletes) adiposity leading to underdiagnosis or overdiagnosis respectively.[49,50] A disease is defined as a distinct pathophysiology that can cause alterations in a single organ or multiple organs. Excess adiposity alone does not satisfy this definition.
Therefore, terms like preclinical and clinical obesity have been recommended in the recent consensus guidelines by F. Robino et al. to address these limitations.[50] Clinical obesity includes alterations in the functions of organs directly caused by excess adiposity and is categorised as a chronic illness, whereas preclinical obesity is characterised by excess adiposity without major signs/symptoms of organ dysfunction due to obesity and is categorised as a physical phenotype and not as a disease.
The recommendations further suggest that a person with increased BMI should be confirmed for having excess adiposity by other anthropometric measurements or by direct body fat measurement. Once confirmed, the next step is to categorise him/her into preclinical or clinical obesity. Clinical obesity is managed like any other chronic disease with evidence-based treatment. Patients with preclinical obesity need regular monitoring for appearance of clinical obesity or other adiposity related diseases, while sometimes requiring treatment when the risk of developing clinical obesity is high or when reducing obesity can help in managing other diseases (certain cancers, transplantation, orthopaedic surgeries, etc.).
Conclusion
With the booming economy, development and urbanisation in South Asia, there is an increased prevalence of sedentary lifestyle, fast food consumption and psychological stress contributing to obesity. Promotion of a healthy lifestyle and eating habits at the level of individual, family, school or workplace and the community as a whole should be encouraged to prevent obesity. Education of the public to recognise obesity as a chronic illness, which if untreated can lead to several health hazards and requires long-term follow-up and care is the need of the hour. Designing an individualised treatment plan, patient education and ensuring adherence to treatment are key elements of management of obesity.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
Not applicable.
Credit author statement
Sambit Das and Amogh Chappalagavi: Conceptualisation, data collection and analysis, literature search, manuscript writing, editing and final approval.
Arun Kumar Choudhury, Dayanidhi Meher, Devadarshini Sahoo, Sandeep Kumar Sahu and Sheenam Gupta: literature search, data collection and analysis, editing and supervision.
Data availability
Not applicable.
Use of artificial intelligence
There was no use of artificial intelligence in preparing this manuscript.