
Abstract
Aim:
The aim of this study was to study intratumoral heterogeneity in the expression of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) between two different cores/blocks of core needle biopsy (CNB), two different blocks of the same lesion in resection specimen (RS), and in between the CNB and RS.
Materials and Methods:
This is a prospective observational study of all the cases of breast carcinoma received in the department of histopathology for 2 years. All the patients with breast carcinoma diagnosed by CNB and RS were analyzed by three pathologists independently by immunohistochemistry.
Results:
Of the 75 cases, 74 were females and 1 male with a peak incidence of 60–70 years. Invasive breast carcinoma of no special type (97%) was the most common, followed by invasive lobular carcinoma (3%). Grade III tumors (44%) were more common, followed by Grade II (39%) and Grade I (17%). ER and PR showed a concordance rate of 96% (P < 0.05), whereas the HER2 showed a concordance rate of 93% (P < 0.05%). The concordance of ER decreased with increasing tumor size and grade, while PR and HER2 showed variable concordance with tumor size and grade.
Conclusion:
The concordance rate of ER and PR (96%) was higher than (93%) HER2. In most cases, biomarker expression in core biopsy and single tumor block was reflective of breast carcinoma as a whole. However, because of the heterogeneous expression of biomarkers, we recommend testing tumors with negative biomarker expression on CNB, again on the RS.
Keywords
Introduction
Breast carcinoma is a major health burden worldwide as it is the second-most common cancer and the leading cause of mortality among women.[1] It is first classified, graded, and then biomarker analysis is done, to understand the nature of the disease for treatment and prognostication purposes. The biomarker analysis of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) is generally performed on core needle biopsy (CNB) and resection specimen (RS) by immunohistochemistry.[2] Endocrine treatment has been shown to significantly increases the overall survival in individuals with biomarker positivity. However, the heterogeneous expression of hormone receptors in tumor tissue has been a confounding factor in the assessment of CNB, and some authors believe that excision biopsy may be a more reliable tissue for assessing the biomarker expression.[3] The concordance of biomarkers status between CNB and RS has been extensively studied in the literature.[3] Breast tumor marker heterogeneity is observed among different patients (intertumoral heterogeneity) and even within individuals (intratumoral heterogeneity) manifesting as spatial or temporal heterogeneity.[4] The heterogeneous expression of biomarkers can occur within a tumor due to different clones or due to improper preservation of specimens and cause discordance between CNB and RS.[2] Hence, the assessment of heterogeneity in the expression of common biomarkers and correlation with morphology may guide us to choose the area for further biomarker study and in deciding whether to repeat the test on the RS or in another block of the CNB. In the present study, we assessed the concordance between two different cores/blocks of CNB, two different blocks of the same lesion in the RS, and in between the CNB and RS when available. This study was done to assess the pattern of expression of ER, PR, and HER2 in different areas of the same tumor.
Materials and Methods
This is a prospective observational study of all cases of breast carcinoma with CNB and RS received in the department of pathology from November 2020 to November 2022. The cases with insufficient material for immunohistochemistry and with poor preservation were excluded from the study.
The CNB and RS were obtained in 10% neutral-buffered formalin, fixed for 6–8 h, and grossed according to the protocol. The tissue was processed overnight, paraffin block sections are made, and the slides were stained with hematoxylin and eosin. A light microscopy study of the morphology was done and classified according to the 2019 World Health Organization classification of the tumors of the breast.[5] Immunohistochemistry for ER, PR, and HER2 was performed and evaluated by three pathologists independently. Immunostaining was performed using Ventana BenchMark XT instrument and determined using primary antibody SP1 Clone for ER, 1E2 Clone for PR, and 4B5 Clone for HER 2. ER and PR were evaluated as per the Allred score methodology of the American Society of Clinical Oncology (ASCO) and the College of American Pathologists (CAP) protocol. The scores of 0 and 2 were negative and scores of 3–8 were positive.[6],[7] HER2 was also reported as per ASCO/CAP protocol, where HER2 overexpression was scored as 0–3+.[6],[7] CNB was compared with RS. Two blocks from different areas of the tumor in RS or two cores from different areas of the tumor in CNB were also compared with each other.
The study protocol was presented to the Institutional Ethical Committee in November 2020 and the IRB number is obtained.
All the continuous variables are represented as mean ± standard deviation. Nonnormally distributed variables are represented by the median (interquartile range [IQR]). Categorical variables are represented by percentages. Comparison of categorical variables was done by the Chi-square test or Fisher's exact test. The coefficient of variation was calculated. All P < 0.05 is considered statistically significant. Data entry was done in Microsoft Excel 2007. Data analysis was carried out by IBM SPSS for Windows Version 25.0, Armonk, NY, USA: IBM Corp.
Results
Seventy-five cases of patients with breast carcinoma were evaluated for intratumoral heterogeneity in the expression of ER, PR, and HER2 during the study period of 2 years. Among these, 74 (98.7%) were female and 1 (1.3%) patient was male. The age range was 32–79 years, with peak incidence at 60–70 years. The tumor characteristics and surgical management are summarized in [Table 1].
Patient and tumor characteristics

For each case, two blocks were taken and compared for receptor expression, which were labeled as Block 1 and Block 2.
Estrogen receptor concordance
Of 75 cases, Block 1 showed ER positivity of 65% (n = 49) and negativity of 35% (n = 26). Block 2 showed ER positivity of 67% (n = 50) and negativity of 33% (n = 25). There were 72 concordant cases and 3 discrepant cases [Figure 1]. The overall concordance rate for ER from two different areas of the tumor was 96% and its P = 0.0000 (<0.05) which is statistically significant [Table 2].
Estrogen receptor and progesterone receptor concordance between different areas of tumor

Example of estrogen receptor (ER) intratumoral heterogeneity between core needle biopsy (CNB) and resection specimen (RS). Case 1: ER is negative in CNB, whereas strongly positive in RS. Case 2: ER shows moderate-to-weak positivity in CNB, whereas negative in RS. (H and E, ×400)

Progesterone receptor concordance
Of 75 cases, Block 1 showed PR positivity of 61% (n = 46) and negativity of 39% (n = 29). Block 2 showed PR positivity of 63% (n = 47) and negativity of 37% (n = 28). There were 72 concordant cases and 3 discrepant cases [Figure 2]. The overall concordance rate for PR from two different areas of the tumor was 96% and its P = 0.0000 (<0.05) which is statistically significant [Table 2].
Example of progesterone receptor (PR) intratumoral heterogeneity core needle biopsy (CNB) and resection specimen (RS). In both Case 1 and Case 2: PR is negative in CNB, whereas strongly positive in RS (H and E, ×400)

Human epidermal growth factor receptor 2 concordance
Of 75 cases, Block 1 showed HER2 positivity of 19% (n = 14), negativity of 69% (n = 52), and 12% (n = 9) were equivocal. Block 2 showed HER2 positivity of 19% (n = 14), negativity of 71% (n = 53), and 10% (n = 8) were equivocal. There were 70 concordant cases and 5 discrepant cases [Figure 3]. The overall concordance rate for HER2 from two different areas of the tumor was 93% and its P = 0.0000 (<0.05) which is statistically significant [Table 3].
Human epidermal growth factor receptor 2 concordances between different areas of tumor

Example of human epidermal growth factor receptor 2 (HER2) intratumoral heterogeneity between core needle biopsy (CNB) and resection specimen (RS). Case 1: HER2 is equivocal in CNB, whereas negative in RS. Case 2: HER2 is negative in CNB, whereas equivocal in RS (H and E, ×400)

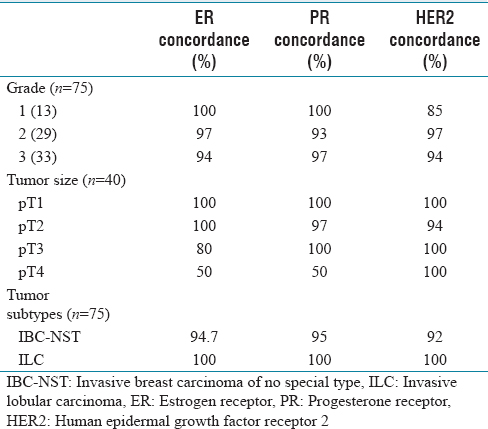
Biomarker concordance with grading, tumor size, and tumor subtypes
ER and PR showed 100% concordance in Grade 1 tumors. As the grade increased, the concordance of ER decreased, but PR showed variable heterogeneity. HER2 showed 85% concordance in Grade 1 tumors. In contrast to ER, as grade increased, concordance of HER 2 also increased.
In pT1 tumors, ER, PR, and HER2 showed 100% concordance. As the tumor size increased, the concordance of ER decreased to almost 50% in T4 tumors, whereas PR and HER2 showed major discordance even in T2 tumors.
The concordance rate of ER, PR, and HER2 in invasive breast carcinoma of no special type (IBC-NST) was 94.7%, 95%, and 92%, respectively, while invasive lobular carcinoma (ILC) had 100% concordance [Table 4].
Receptor concordance with grading, tumor size, and tumor subtypes
Discussion
Breast carcinoma is a heterogeneous disease with phenotypic and genetic intratumoral heterogeneity.[4] CNB is a reliable method for diagnosing breast cancer and assessment of biomarkers expression, which is essential for providing systemic therapy and neoadjuvant chemotherapy. It is the only data available before primary systemic treatment and is considered a gold standard for preoperative assessment. However, the conflicting evidence available in terms of concordance in evaluation between CNB and RS leads to different recommendations concerning the use of CNB for biomarker testing.[3] In the present study, we assessed the concordance between two different cores/blocks of CNB, two different blocks of the same lesion in the RS, and between the CNB and RS. This study was done to assess the expression of ER, PR, and HER2 in different areas of the same tumor.
Clinical characteristics
The incidence of breast carcinoma increases with age. In our study, the peak incidence was at 60–70 years, where 68% of tumors were above the age of 50 years. The study by Chopra et al. showed a peak incidence at 41–50 years, with 60% below the age of 50 years.[8] IBC-NST is the most common subtype, followed by ILC in our study, which is comparable to the study by Lorgis et al. and Clark et al.[2],[9]
In our study, Grade 3 tumors were more common, followed by Grade 2 and Grade 1 tumors, similar findings are found by Meattini et al.,[10] however, some other studies show a preponderance of Grade 2 tumors.[2],[11]
Estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 concordance
The concordance rate of ER and PR in previous literature varies from 83% to 99% and 78.3% to 95%, respectively[2],[10],[11],[12],[13],[14],[15],[16],[17],[18] [Table 5]. In our study, the concordance of ER and PR between two different areas of the tumor was 96% each, which is similar to the study done by Jeong et al.[11] The concordance of ER was higher than PR in some studies, due to increased heterogeneity of PR expression within the tumor.[11],[12] However, our study showed a similar concordance rate for ER and PR.
Concordance of estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 between different areas of tumor

We had three discrepant cases of ER and PR expression assessed by three pathologists independently thus excluding subjective interobserver variability. The variation of biomarker expression within the same tumor is notable because of intratumoral heterogeneity, therefore, the tumor area with a phenotypically distinct cell population was not diagnosed during initial tumor subtyping in the CNB, leading to relapse.[19] However, the PR discordant tumors in our study were ER-positive and, therefore, were eligible for hormonal therapy.
Studies in the literature show variable HER2 concordance ranging from 75.4% to 96.8% [Table 5].[2],[10],[11],[12],[13],[14],[15],[16],[17],[18] In our study, the concordance of HER2 between two different areas of the tumor was 93%. Studies done by Chen et al. and Asogan et al. show slightly higher concordance rates of 96.3% and 96.8%, respectively.[13],[14]
Since intratumoral heterogeneity is inevitable, we suggest repeating testing on cases that are biomarker negative in CNB and those with morphological discordance. Since CNB represents only a small portion of the tumor, the overall biomarker expression may always not be representative of the entire tumor.
Comparing the receptor concordance with tumor grade, tumor size, and subtypes
As tumor grade and size increased, the concordance of ER decreased in our study, similar to the study done by Kombak et al. However, PR and HER2 show variable concordance in the present study.[20] ILC shows a higher concordance rate for ER, PR, and HER2 compared to IBC-NST, which is also comparable to the findings by Kombak et al.[20]
Limitations
Due to financial limitations, the study was not strengthened with molecular techniques such as fluorescence in situ hybridization (FISH), especially in equivocal cases. Many cases with core biopsies after diagnosis had resection elsewhere, and cases only with RS s had previous biopsy elsewhere, hence could not be studied extensively. Due to the pandemic situation, the number of resection cases was also reduced and distributed elsewhere due to a lack of accessibility because of the lockdown.
Conclusion
We conclude that the expression of biomarkers in two different areas of the same tumor was concordant in the majority of the cases. The concordance ER and PR (96%) were slightly higher than HER2 (93%). In most cases, the biomarker expression on CNB or single tumor block in RS is reflective of breast carcinoma as a whole and is sufficient for clinical decision-making. However, some heterogeneity in the expression of these biomarkers exists, this might be a cause for false-negative results on the CNB. Hence, we recommend retesting biomarker expression study in tumors which were negative in CNB on the RS, as these patients may benefit from the targeted therapies. As the concordance rate of HER2 is less, molecular techniques such as FISH are recommended in HER2-negative and equivocal cases.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
IRB number is obtained and approved by Institutional Ethics Committee - Biomedical Research Apollo Hospitals, Chennai - AMH-DNB-032-11-20.
Funding
Nil.
Author's contribution
Dr. Ragavi Uthayasuriyan: Conception of the idea, data acquisition, data analysis, statistical analysis, drafting the article, and submission, Dr. Sheba K Jacob: Conception of the idea, data analysis,critical revision of the manuscript, and final approval of the version to be published, Dr. Saloni Naresh Shah:Data analysis, critical revision of the manuscript and final approval of the version to be published.