
Abstract
Background:
Acne vulgaris is a common disorder of pilosebaceous units affecting adolescents and young adults. The various causes include diet, stress, seborrhea, and premenstrual flare.
Objective:
The objective of this study was to compare lipid profile, insulin, and adiponectin levels in acne and controls.
Materials and Methods:
Sixty patients of acne from the age group of 12 to 25 years and 20 healthy age- and gender-matched controls were included in the study.
Results:
Patients with acne showed significantly higher levels of total cholesterol and low-density lipoprotein (LDL), higher levels (although not statistically significant) of triglyceride, and very LDL and significantly lower levels of high-density lipoprotein as compared to controls. Furthermore, individuals with acne had significantly lower levels of serum adiponectin and significantly higher mean levels of fasting serum insulin as compared to controls.
Conclusion:
Derangements in serum lipid profile, serum insulin, and serum adiponectin levels can predispose to acne in adolescent individuals. Thus, dietary and lifestyle modifications should be recommended in such patients.
Introduction
Acne vulgaris is a common disorder of the pilosebaceous unit, which manifests as comedones, papules, pustules, nodules, and varying degrees of scarring. Individuals of all age groups can be affected, particularly adolescents, i.e., those between 15 and 17 years of age.[1],[2]
High-glycemic diet, obesity, high body mass index (BMI), and stress play an important role in the aggravation of acne vulgaris. Various metabolic derangements affect the occurrence of acne in different ways.
Insulin causes increased sebum production by increasing the bioavailability of androgens.[3] This is done by inducing the production of androgens and inhibiting the hepatic synthesis of sex hormone-binding globulin.[4] Furthermore, hyperinsulinemia increases serum levels of insulin-like growth factor 1 (IGF-1) and reduces serum levels of IGF-binding protein 3, leading to the proliferation of keratinocytes and comedone formation.[5]
Lipid profile abnormality such as increase in total cholesterol (TC) and low-density lipoprotein (LDL) and a decrease in high-density lipoprotein (HDL) affects the occurrence of acne vulgaris by increasing androgen levels, as androgens are synthesized from cholesterol.[6]
Adiponectin is a protein hormone produced exclusively by adipocytes that regulates the metabolism of lipids and glucose. It increases insulin sensitivity, decreases proinflammatory cytokines, and increases anti-inflammatory ones.[7] The association of low adiponectin levels with obesity, insulin resistance, and coronary artery disease indicates that this novel protein may be an important new marker of metabolic syndrome.[8],[9] Furthermore, its role is being evaluated in many dermatological disorders associated with metabolic derangements such as psoriasis, acanthosis nigricans, and androgenetic alopecia. This prompted us to look for its role in the pathogenesis of acne.
Materials and Methods
For this cross-sectional study, 60 cases of acne, in the age group of 12–25 years, visiting the skin outpatient department of a tertiary care center in Punjab were recruited. Twenty age- and gender-matched healthy controls were taken.
Patients not willing to take part in the study, those on treatment for acne or any other drugs likely to interfere with lipid profile, smokers, alcoholics, patients with polycystic ovary syndrome (PCOS)/other hormonal disturbances, and patients with a history of familial hyperlipidemia or metabolic syndrome were excluded from the study.
The study was started after taking informed consent from patients and approval from our institution's ethics committee.
At the initial visit, each patient's detailed history and clinical examination were conducted. Patients suspected to have PCOS/androgen derangement were tested for the same and excluded from the study. BMI was calculated as weight (kg)/height (m2). Acne cases were classified into the following three categories according to the international consensus conference: mild (few to several comedones, papules, and pustules; no nodules), moderate (several comedones, papules, and pustules; few to several nodules), severe (numerous comedones, papules, and pustules; many nodules).[10] Then, each participant was tested for serum insulin levels, lipid profile, and adiponectin levels.
Statistical analysis
Statistical analysis was performed using SPSS software version 22 (SPSS Inc., Chicago, Ill., USA). Results were described as mean ± standard deviation. The significance of mean difference among groups was compared using Student's t-test, Chi-square, and Fisher's exact test. A P < 0.05 was considered statistically significant. For comparing more than two mean groups, one-way anova test was used.
Results
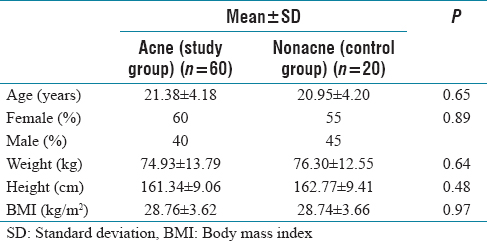
A total of 80 (60 acne and 20 nonacne) age-, sex-, and BMI-matched patients in the age group of 12–25 years were enrolled in the study [Table 1]. The mean age of acne patients and controls was 21.38 ± 4.18 years and 20.95 ± 4.20 years, respectively, which was comparable. The age of patients ranged from 15 to 24 years, whereas in the control group, it ranged from 14 to 22 years. In the patient group, there were 36 females and 14 males, whereas in controls, there were 11 females and 9 males. According to severity, acne patients were grouped into mild (20 cases or 33.3%), moderate (30 cases or 50%), and severe (10 cases or 16.6%).
Demographic parameters of the study participants
Acne patients showed higher levels of TC (192.03 ± 18.65), triglyceride (TG) (121.58 ± 46.34), LDL (113.43 ± 19.36), and insulin (14.62 ± 9.1) and lower levels of HDL (43.41 ± 8.23) and adiponectin (8.56 ± 2.7) than controls. The difference in these values among both groups was statistically significant [Table 2].
Comparison of parameters among individuals in the study and control group

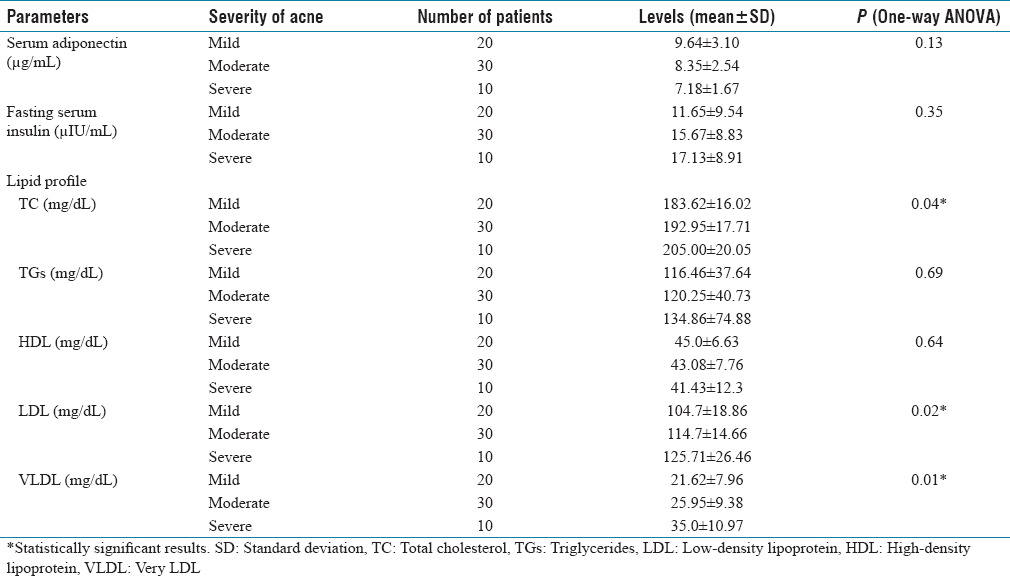
When going from mild-to-severe acne, the mean difference in levels of TC (P = 0.04), very LDL (VLDL) (P = 0.01), and LDL (P = 0.02) was statistically significant. Although higher mean levels of TG and insulin and lower mean levels of HDL and adiponectin were present in severe acne cases as compared to mild acne, the difference was not statistically significant [Table 3].
Evaluation of parameters with severity of acne among individuals in study group
Discussion
Acne vulgaris is a multifactorial disease of the pilosebaceous unit affecting particularly adolescent age group. Four key pathogenic processes lead to the formation of acne lesions: (1) follicular hyperkeratinization, (2) increased and altered sebum production under androgen control, (3) proliferation of Propionibacterium acnes, and (4) inflammation. Various metabolic derangements are known to be associated with acne. The relationship of acne with lipid profile, insulin, and adiponectin levels has shown mixed results in various studies and is not widely reported.[10],[11] The aim of the present study was to compare the lipid profile, serum insulin levels, and serum adiponectin levels among individuals with and without acne.
In the present study, the mean age in the acne group was 21.38 ± 4.18 years, and in controls, it was 20.95 ± 4.20 years [Table 1]. The mean BMI of cases was 28.76 ± 3.62 and controls were 28.74 ± 3.66, which was comparable. Higher BMI was due to dietary and lifestyle habits in our geographical area. According to the severity of acne, the most common type was moderate acne, found in 50% of individuals with acne, followed by mild (33.3%) and severe (16.6%) types.
It has been reported in different studies that derangement in one or more parameters of the lipid profile is associated with the causation of acne.[12],[13],[14] In our study, significantly higher levels of TC (P = 0.0001), LDL (P = 0.001), and significantly lower levels of HDL (P = 0.01) were present among patients with acne compared to the control group. Although not statistically significant, higher levels of TG (P = 0.06) and VLDL (P = 0.53) were seen in patients with acne compared to control group patients. Akawi et al.[12] and Abulnaja[13] found that acne patients had significantly low plasma HDL levels. They also reported significantly higher levels of TGs and LDL in patients with severe acne compared with those in healthy controls. Akawi et al.[12] noticed a trend of derangement in the lipid profile of acne patients with acne severity. We also observed a similar trend in derangement of TC (P = 0.04), LDL (P = 0.02), and VLDL (0.01) with increasing severity of acne from mild to moderate and mild to severe [Table 3]. Our study is also in harmony with the study done by Bakry et al.[14] and Da Cunha et al.[15] where they found significantly higher levels of TC and significantly lower levels of HDL cholesterol in patients with acne. This point toward the possibility of the positive association between the pathogenesis of acne and lipid derangements.
Decreased adiponectin levels are thought to play a central role in the development of type 2 diabetes, obesity, and cardiovascular disease in humans. Recent evidence has indicated that adiponectin has a causal role in the pathophysiology of several skin diseases as well. The dysfunction of lipid synthesis (which is regulated by adiponectin) in sebaceous glands may be a contributor to the pathogenesis of acne. In the present study, levels of serum adiponectin were found to be significantly lower in acne patients as compared to the control group [8.56 ± 2.7 vs. 10.08 ± 5.9 μg/mL, P = 0.03, [Table 2]]. However, adiponectin levels did not vary significantly with an increase in the severity of acne. [P = 0.13, [Table 3]] This result is comparable to studies done by Kovács et al.,[16] Aydin et al.,[17] and Çerman et al.[10] Results of Ozuguz et al.[18] differ from our study, where no statistically significant difference in serum adiponectin levels were found among study individuals.
We also found higher serum insulin levels among acne patients compared to the control group [14.62 ± 9.1 vs. 9.99 ± 6.47 μIU/mL, P = 0.01, [Table 2]]. There was a trend toward increase in serum insulin levels with an increase in acne severity (although not significant, P = 0.35), which points toward the association of insulin resistance with the pathogenesis of severe acne. Emiroğlu et al.[11] and Abulnaja[13] found that fasting insulin levels were significantly higher in the acne patients than in the control group. Hence, our results were in agreement with the above studies. Munichandrappa et al.[19] did not find any statistically significant difference in fasting insulin levels between cases and controls (although levels were higher in acne cases as compared to the control group). This is contradictory to the results of our study. However, as seen in our study, they observed a weak positive correlation between acne severity and fasting insulin levels.
Conclusion
We can conclude that along with derangements in other metabolic parameters (lipid profile and insulin), decreased adiponectin level may be another pathogenetic cofactor that augments the inflammatory response in patients with acne vulgaris. Our study being time-bound could not assess the role of drugs such as metformin and isotretinoin on above-mentioned parameters. Metformin increases insulin sensitivity, whereas isotretinoin has been shown to increase adiponectin levels.[17] Hence, more studies are needed to evaluate the role of these drugs as an adjunct therapy in severe acne. Furthermore, dietary and lifestyle modifications should be recommended in such patients because of the beneficial metabolic and immunologic effects.
Limitation
Small sample size owing to the high cost of the test kit
BMI was toward the upper limit because of faulty eating habits and the sedentary lifestyle of adolescents these days.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Institutional ethical committee approval
The study was conducted after taking clearance from the Institutional Ethical Review Committee. {(Trg).EC/NEW/INST/2017/197/10364}.
Funding
Nil.
Author's contribution
SA, AS and DC are the Principal Investigators who conceived the study. JB, AS, SG and DC designed the study; SA and PC contributed to the literature searches and review; JB, AS, SG and DC were involved in data collection; SA, SG and PC carried out data analysis; SA, JB, AS and SG wrote the manuscript; SA, JB and DC provided the critical revision of the manuscript for important intellectual content; all authors have read and approved the final manuscript.