
Abstract
Objective:
Olanzapine is an atypical antipsychotic medication and known for metabolic side effects but olanzapine-induced obsessive–compulsive symptoms are another important behavioral side effects which are less studied and only a few case reports reported these side effects. This study aims to estimate the prevalence and pattern of olanzapine-induced obsessive–compulsive symptoms in schizophrenia and bipolar affective disorders (BPADs).
Methods:
Subjects were recruited from psychiatry outpatient department. Subjects with schizophrenia (n = 41) and BPAD (n = 18) taking olanzapine at least more than 6 months were evaluated for clinical profile and the presence of obsession and compulsion symptoms by means of Yale-Brown Obsessive–Compulsive Symptom (YBOCS) checklist scale and data were collected on the structured format.
Results:
Eighteen (30.5%) of the 59 patients met YBOCS checklist scale for both obsessive–compulsive symptoms among subjects with schizophrenia and BPAD subjects. The mean duration of olanzapine intake was 2 years and the mean dose of olanzapine was 12.5 ± 5.21 mg in obsessive–compulsive symptoms (OCSs) present subjects and the mean dose was 13.78 ± 5.21 mg in subjects not having OCSs. Contamination was the most common obsession and checking was the most common compulsion.
Conclusions:
These findings suggest that obsessive–compulsive symptoms occur in a substantial percentage of patients taking olanzapine in schizophrenia and BPAD and most of the subjects had more than one OCS.
INTRODUCTION
Olanzapine is a thienobenzodiazepine classified as an atypical second-generation antipsychotic agent and indicated for acute and maintenance treatment for schizophrenia, bipolar disorder, and use as an adjunctive agent in the treatment resistance depression.[1,2]
Atypical antipsychotic emergent important adverse effects are weight gain, impaired blood sugar, deranged lipid profile, and medication-induced obsessive–compulsive symptoms (OCSs), especially with clozapine and olanzapine.[3] While behavioral side effects, such as medication-induced OCS, receive less attention and significance than physical side effects in routine clinical practices. The current evidence shows that schizophrenia patients with OCS display a worse clinical course, poor treatment response, worse long-term outcome, and greater prefrontal cortex functional impairments.[4,5] Similarly, in bipolar disorder, OCS accounted for 21% of all comorbidities.[6] OCS presence in bipolar disorder results in an increased occurrence of depressive episodes, elevated suicide rates, more frequent hospital admissions, heightened chronic episode occurrence, and lingering residual symptoms.[7]
The presence of OCSs in schizophrenia and bipolar disorder is associated with a negative impact on the general prognosis of the illness. Atypical antipsychotics are widely used in the treatment of schizophrenia and in comparison to clozapine, and olanzapine is a more consumed medicine than clozapine because clozapine is exclusively used in treatment-resistant schizophrenia and in few special conditions.[8] Therefore, the magnitude of medication-induced OCS much higher with olanzapine in comparison to clozapine. To the best of our knowledge, no study has assessed the prevalence of OCS in a group of schizophrenia and bipolar disorder patients. Studying the magnitude and pattern of olanzapine-induced OCS is necessary to improve early detection and prevent its negative impact on the prognosis of schizophrenia and bipolar disorder.
METHODS
Subjects study design and sample
A cross-sectional study was designed and ethical approval was obtained from the institutional ethical committee. Data were collected from the outpatient clinic of the psychiatry department. Eligible participants for the study were included after obtaining written informed consent. Patients diagnosed with schizophrenia or bipolar disorder according to ICD-10 who had been taking olanzapine for over 6 months were included in the study. The recruitment of subjects was carried out through a simple random sampling method and data were collected over 6 months. Assessments were performed through face-to-face interviews and clinical examinations conducted on the same day in the outpatient department.
Tools
Data were collected on a specifically designed pro forma to record sociodemographic and clinical details such as comorbid medical illness, history of alcohol use, duration of olanzapine intake, dose of olanzapine, duration of illness, and family history. Assessments of OCS were done with Yale-Brown Obsessive–Compulsive Symptom (YBOCS) checklist and the presence of OCS in study subjects grouped in OCS present and absent.
Statistical analysis
Data were entered into MS Excel spreadsheet and analysis was done using the IBM Statistical Package for the Social Sciences (SPSS) version 21.0. Means with standard deviations and frequencies with percentages were used to summarize continuous and categorical variables, respectively. Student’s t-test (continuous variables) and Chi-square test (categorical variables) were used for comparative analyses. For all analyses, the level of significance was set at P < 0.05.
RESULTS
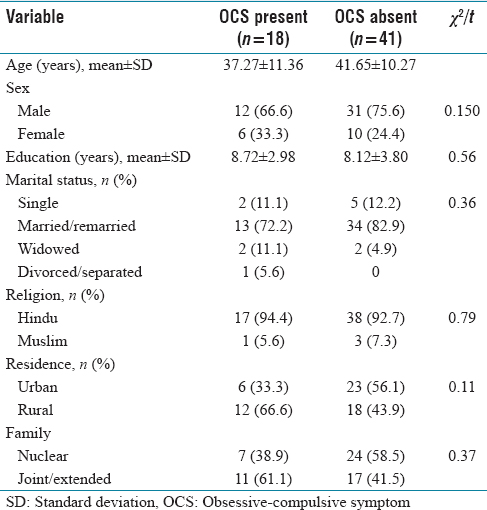
The baseline characteristics of the subjects with OCS and subjects with absent OCS are shown in Table 1.
Sociodemographic profile
Sociodemographic profile
A total of 59 subjects were enrolled in the study and assessed by clinical examinations and the YBOCS checklist. There were 72.9% (43) male and 17.1% (16) female study subjects and the mean age of study subjects was 40.3 ± 10.7 years. Most of the study subjects were married and belonged to Hindu religions. Sociodemographic characteristics of subjects with OCS and subjects with absent OCS were not shown statistically significant differences.
Clinical characteristics
The study sample consists of 69.4% (41) schizophrenia and 30.6% (18) bipolar affective disorder (BPAD) patients. The mean duration of illness was 9.9 ± 6.5 years and mean dose of olanzapine was 13.4 ± 5.2 mg and comorbid medical illness was 6.7% (4) of study subjects [Table 2].
Clinical profile of study sample

Obsessive–compulsive symptoms
Application YBOCS symptom checklist among subjects who had OCS shows that obsession was presented in 8 subjects and compulsion was noted in 10 subjects. Contamination and aggressive obsession were the most common obsession and checking was the most common compulsion. Among 18 subjects having OCS, 7 subjects have 2 OCS and 3 subjects have 3 OCS [Table 3].
Obsessive-compulsive symptom dimension in the study sample

DISCUSSION
The purpose of this study was to determine the frequency of obsessive–compulsive disorder in schizophrenia patients with the use of structured interviews and standardized diagnostic criteria. Epidemiologic studies have estimated the prevalence of OCD is 2% in the general population, up to 4% in general psychiatric inpatient setting.[9,10] The recent literature has suggested that the frequency of prominent OCS in schizophrenia is around 25% and 11%–21% of persons with bipolar disorder at some time during their bipolar disorder.[11,12] In this study, the overall prevalence of OCS in the study sample was 30.5%, the prevalence of OCS in schizophrenia subjects was 29.26%, and 33% in BPAD subjects. The prevalence of obsession was 45% and compulsion was 55%. More than half subjects had more than one OCS, and checking was the most common compulsion, aggression, and contamination was the most common obsession. OCS is common in schizophrenia. The treatment of emergent obsessive–compulsive symptoms has raised concern since the widespread introduction of serotonin-dopaminergic antagonists.[13] Olanzapine is an atypical antipsychotic agent with a dual antagonistic effect on 5-HT2 and D2 receptors and may lead to serotonin-dopamine imbalance and thus leading to treatment of emergent OCD.[14] The concomitant drugs used alongside olanzapine were benzodiazepines and trihexyphenidyl, which had no impact on OCS emergence or the OCS profile.
Hence, there is a need for routine screening and close monitoring for the emergence of OCS among patients receiving of olanzapine and manage them appropriately to prevent negative impacts of olanzapine emergence of OCS in schizophrenia and BPADs.
CONCLUSION
Study findings suggested that obsessive–compulsive symptoms occur in a substantial percentage of patients taking olanzapine in schizophrenia and BPAD and most of the subjects had more than one OCS.
Limitations
The sample size was small. A larger sample size could add power to the study.
Several other factors such as birth order and family history of history OCS were not studied.
The severity of psychotic or mood symptoms and other adverse effects due to olanzapine was not taken into consideration in the study.
At baseline or drug-naïve stage, the prevalence of OCS was not included in the study.
Implications
The emergence of OCS during the treatment of schizophrenia and bipolar disorder causes negative consequences in course, outcome, and responsiveness to medications. Olanzapine emergence of OCS is a behavioral side effect of medications such as other physical side effects of olanzapine, for example, weight gain. Early recognition of medication-induced OCS is helpful to avoid the negative consequences of olanzapine-induced behavioral side effects. We should promote education about the behavioral side effects of psychotropic medications, responsible use, and supervision of medication-induced behavioral side effects in patients so that problem should be identified earlier and managed accordingly.
Footnotes
Conflicts of interest
There are no conflicts of interest.
Informed consent
Written informed consent was obtained.
Funding
Nil.
Author’s contribution
DKM, UPS, VN, AK conceptualize, design, and write the manuscript.