
Abstract
Although hypoxic pulmonary vasoconstriction is a well-recognized physiological phenomenon it is unusual to observe and assess its efficiency in clinical practice. Here, we report the case of a 50-year-old female who presented with unilateral incomplete bronchial occlusion due to a carcinoid tumor involving the left main bronchus in the absence of atelectasis. Ventilation-perfusion imaging revealed absent ventilation and perfusion to the left lung. She underwent bronchotomy and removal of the tumor. One month after the operation a further ventilation-perfusion lung scan revealed complete restoration of ventilation to the left lung and almost complete recovery of the perfusion. This unusual case demonstrates the marked efficiency of hypoxic pulmonary vasoconstriction at the level of a single lung and its reversible nature following relief of regional hypoxia.
INTRODUCTION
The first systematic description of hypoxic pulmonary vasoconstriction is widely attributed to von Euler and Liljestrand.[1] These investigators were also the first to suggest that this phenomenon serves to protect individuals from systemic hypoxemia by reducing venous admixture from poorly ventilated regions of the lung. The efficiency of hypoxic vasoconstriction varies between species and between individuals.[2–4] In populations residing for generations at a high altitude, where excessive hypoxic pulmonary vasoconstriction would be detrimental, the response is often minimal. In addition, the magnitude of the response has been reported to be greater in small lung regions and weaker if a larger proportion of the lung is hypoxic.[2] Most experimental reports of the efficiency of hypoxic pulmonary vasoconstriction in Man have been necessarily limited to a time course of minutes in normal subjects.[4,5] Here we report an unusual clinical case that demonstrates almost complete, reversible, redistribution of blood flow in an entire lung.
CASE REPORT
A 50-year-old Caucasian female presented to the Accident and Emergency Department for evaluation of acutely worsening breathlessness of seven days' duration, with a background of chronic shortness of breath for the past few weeks. Her primary care practitioner had initiated an inhaled beta-2-receptor agonist, because of suspected asthma, with no benefit. She also felt more breathless when lying on her left side associated with mild chest discomfort. On chest auscultation she was noted to have reduced breath sounds in the left hemithorax, but her presenting chest radiograph was normal [Figure 1a].
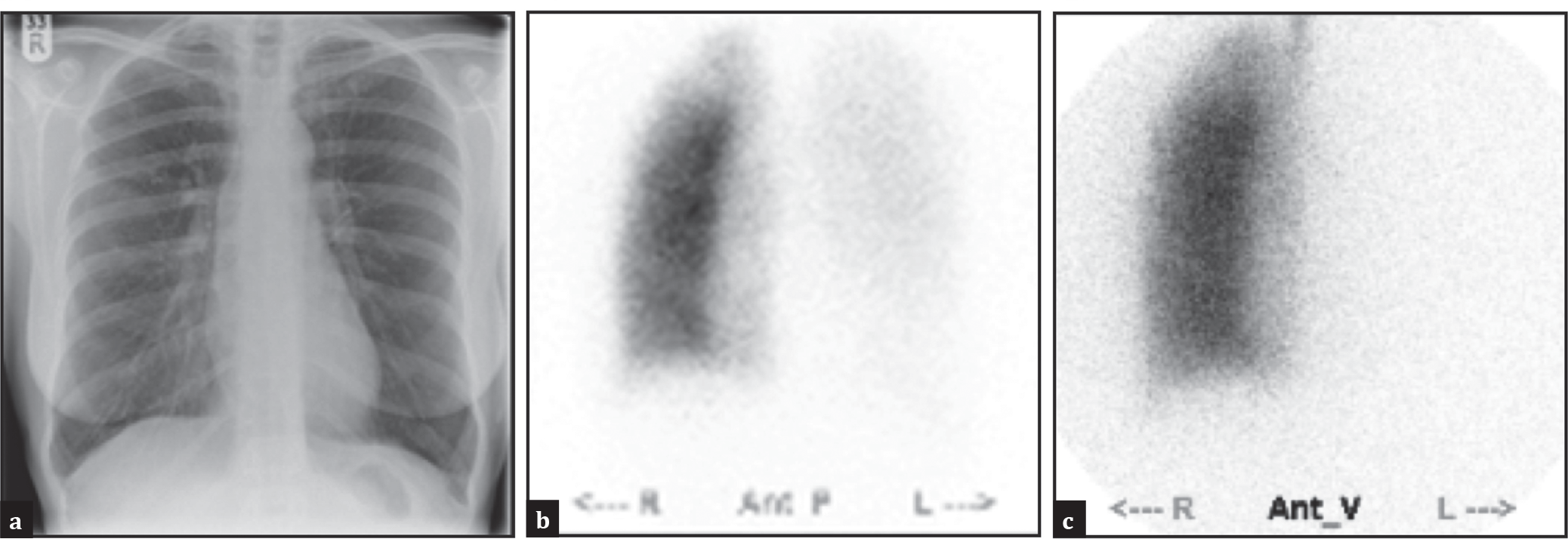
Chest radiograph (a) anterior perfusion and (b) ventilation; (c) lung scintigrams demonstrating loss of ventilation and perfusion to the left lung at initial presentation
She had never smoked. She denied any significant family history. Vital signs were within normal limits and oxygen saturations were greater than 95%. Initial investigations, including full blood count and electrolytes, were normal. Although, when rising from the examination couch, she suddenly complained of severe shortness of breath and chest pain, with oxygen saturations falling to 89%. An urgent ventilation-perfusion (VQ) lung scintigram was arranged to exclude pulmonary embolism. The VQ scan showed complete absence of ventilation and perfusion to the left lung [Figure 1b and c].
In view of the striking findings on the VQ scan an urgent computed tomographic (CT) scan of the chest was performed, which revealed a mass obstructing the left main bronchus close to the origin. There was no evidence of atelectasis on the CT. Bronchoscopy was undertaken the following day, which confirmed the CT findings and identified a fleshy mass almost completely occluding the lumen of the left main bronchus. Biopsies were taken, histology of which were consistent with a bronchial carcinoid tumor.
Two hours after bronchoscopy she became more breathless and her oxygen saturation fell to 85%. A repeat chest radiograph now showed complete collapse of the left lung. She was referred to Papworth Hospital for urgent thoracic surgical assessment. It was decided that the carcinoid tumor was amenable to resection by bronchotomy, involving removal of a segment of the left main bronchus involved with the tumor. This procedure preserved the distal lung without need for pneumonectomy. The operation was successful with complete resection of the tumor and re-expansion of the atelectatic lung. She made an uneventful recovery from surgery.
One month later she attended for follow-up and was virtually symptom-free. A repeat chest radiograph [Figure 2a] showed the presence of surgical staples at the site of bronchial anastomosis, but otherwise normal lung fields. A repeat VQ scan showed almost complete recovery of ventilation and perfusion to the left lung [Figure 2b and c].
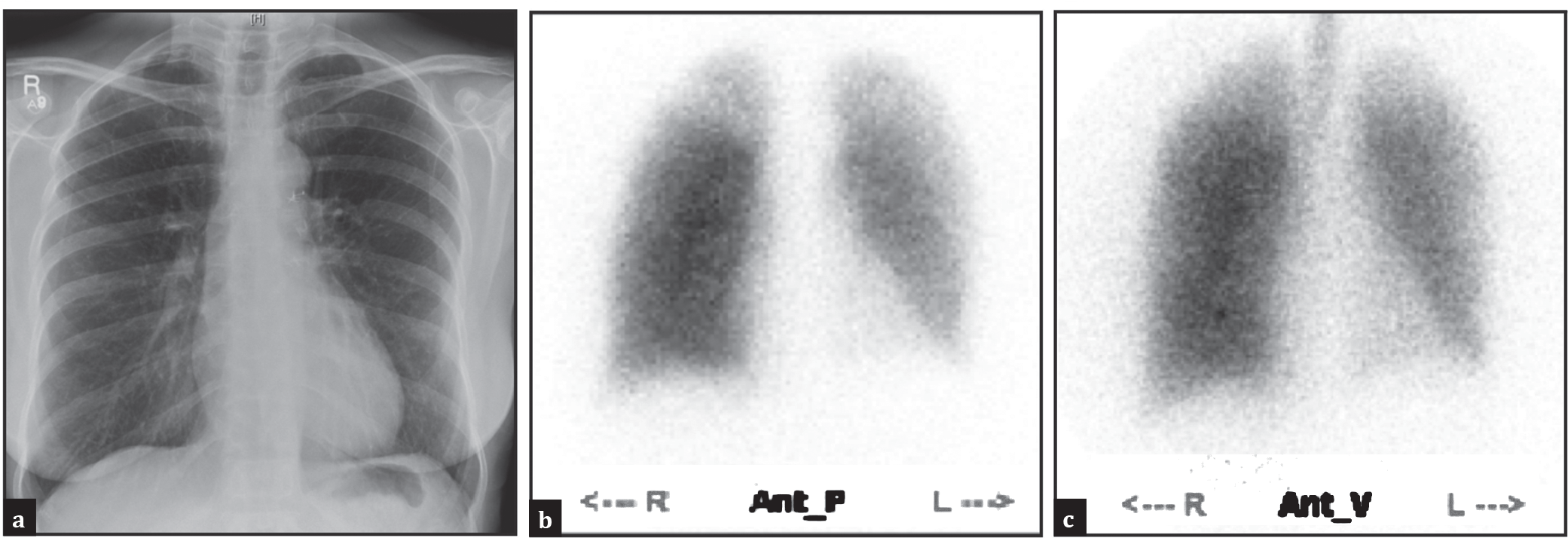
Chest radiograph (a) anterior perfusion and (b) ventilation; (c) lung scintigrams demonstrating restoration of ventilation and perfusion to the left lung one month following surgery
DISCUSSION
The case we describe is unusual in that the patient presented initially with almost complete obstruction of the left main bronchus due to an endobronchial carcinoid tumor, but without associated atelectasis. Atelectasis occurs when the ventilation-perfusion ratio falls to a level at which the rate of gas removal by the blood flow exceeds the rate of gas entering the obstructed lung.[6] Our patient must have had a critically low ventilation-perfusion ratio in the left lung at presentation with an alveolar PO2 that would have approximated mixed venous PO2. This would have provided the stimulus for hypoxic pulmonary vasoconstriction. Although we do not know how long this situation has been present — as a carcinoid is a slow growing tumor — it is likely that the hypoxic stimulus may have been present for some weeks. One can expect a degree of chronic hypoxic vascular remodeling to have occurred under these circumstances. The efficiency of hypoxic pulmonary vasoconstriction can be judged from the lung scintigrams to be nearly complete, in that there has been an almost complete absence of perfusion to the left lung and her peripheral oxygen saturation has been initially measured at greater than 95%. In the absence of this response she may have suffered marked systemic hypoxemia.
Following bronchoscopy and biopsy the obstruction of air flow to the left lung was further compromised and atelectasis occurred, prompting surgical referral and intervention.
At a follow-up one month after surgery the repeat lung scintigram revealed matched restoration of ventilation and blood flow to the left lung. Thus, despite a period of several weeks of hypoxic pulmonary vasoconstriction, probably associated with some chronic pulmonary vascular remodeling, the relief of alveolar hypoxia allowed restoration of blood flow to the left lung. Reversal of both acute and chronic hypoxic vasoconstriction and remodeling is reported in animal models, but rarely observed in clinical practice.