
Abstract
The molecular mechanisms of pulmonary arterial hypertension (PAH) remain ill-defined. The aims of this study were to obtain sequential endoarterial biopsy samples in a surgical porcine model of PAH and assess changes in histology and mRNA expression during the disease progression. Differentially expressed genes were then analyzed as potential pharmacological targets. Four Yucatan micro-pigs underwent surgical anastomosis of the left pulmonary artery to the descending aorta. Endovascular samples were obtained with a biopsy catheter at baseline (before surgery) and from the left lung 7, 60, and 180 days after surgery. RNA was isolated from biopsy samples, amplified and analyzed. Dysregulated genes were linked to drugs with potential to treat or prevent PAH. With the development of PAH in our model, we identified changes in histology and in the expression of several genes with known or investigational inhibitors and several novel genes for PAH. Gene dysregulation displayed time-related variations during disease progression. Endoarterial biopsy provides a new method of assessing pulmonary vascular histology and gene expression in PAH. This analysis could identify novel applications for existing and new PAH drugs. The detection of stage- and disease-specific variation in gene expression could lead to individualized therapies.
Pulmonary arterial hypertension (PAH) is an occlusive disease of the pulmonary arteries which leads to right heart failure and premature death. Despite new therapies, the yearly mortality continues to be about 15%,[1] and the 5-year survival remains around 50-60%.[2,3] The molecular mechanisms of PAH are under investigation. Pulmonary arterial endothelial cells and smooth muscle cells are intimately involved in the development of PAH.[4] Endothelial cell apoptosis and dysfunction[5] and smooth muscle cell hyperproliferation lead to vascular thickening and increased pulmonary vascular resistance. Identified molecular abnormalities linked to PAH include the following: Endothelin-1, serotonin, serotonin transporter, thromboxane, nitric oxide synthase, prostacyclins, potassium channels, bone morphogenetic protein (BMP) signaling and survivin.[6] The inaccessibility of pulmonary vascular tissue has limited studies attempting to better define the mechanisms of PAH. In this study, we utilized a minimally invasive method to obtain endovascular samples coupled with recently developed mRNA expression analyses to enhance our understanding of PAH in a swine surgical shunt model. The dysregulated transcriptome map was then analyzed for potential pharmacologic candidates that could target these molecular abnormalities.
MATERIALS AND METHODS
Swine
Chronic PAH was created in four Micro Yucatan female swine by surgical anastomosis of the left pulmonary artery (LPA) to the descending aorta.[7] Mean body weight was 22.4 ± 5.3 kg and mean age at surgery was 7.3 ± 2.7 months. University of Nevada, Las Vegas, RMED-0804-192 an institutional committee approved the protocol.
Anesthesia, catheterization, and biopsy
Anesthesia was induced and maintained with inhaled isoflurane (Baxter Healthcare Co. Deer Field, IL, USA) as described previously.[7] A baseline right-sided cardiac catheterization with pulmonary angiography was performed through a sheath in the right internal jugular vein. The biopsy procedure was performed as described previously. [8,9] To obtain biopsies, an 8F long sheath was wedged in 2- to 3-mm peripheral pulmonary arteries. At least eight biopsy samples were obtained at each procedure: Two for histologic examination; two for RNA analysis; and four saved for future studies. Catheterization with aortic and LPA pressure measurement, angiography and biopsies of the LPA were performed through an 8F sheath in the carotid artery 7, 60, and 180 days after surgery. Angiograms in distal LPA branches were performed before and after biopsy.
Shunt model
A left thoracotomy was performed in the fourth intercostal space. The LPA was ligated at its origin from the pulmonary trunk. The descending thoracic aorta was clamped and a window was created in its medial aspect with a 4.5 mm punch. An end-to-side anastomosis was created. The chest was closed. No chest tubes were placed. Postoperative care was as described previously.[7]
RNA microarray
Biopsy samples were placed in RNA later and analyzed by Affymetrix GeneChip® Porcine Genome Array, which provides comprehensive coverage of the Sus scrofa transcriptome, containing 23,937 probe sets for 20,201 genes. The sequence information was selected from UniGene Build 28, GenBank® mRNAs, and GenBank® porcine mitochondrial and rRNA sequences. Specimens were homogenized using QIAshredder columns in a FastPrep FP120 Homogenizer. RNA was isolated using RNeasy Mini columns and quantified initially by UV spectrophotometry and more definitively by capillary electrophoresis on an Agilent 2100 Bioanalyzer.
Gene expression analysis and molecular pathways
Gene expression levels were compared between biopsy samples from normal pulmonary arteries at baseline and distal LPA branches after the development of PAH. Data processing and statistical analysis were performed using R/Bioconductor and GeneSpringGX. Molecular pathways were examined using Ingenuity Pathway Analysis. GeneSpringGX was used to assess differential gene expression and perform tests by clustering. Gene expression fold changes for 7, 60, and 180 days postsurgery relative to baseline were then loaded into specially written Kolmogorov-Smirnov statistical scripts to compare the PAH genes to genes previously known to be affected by certain drugs.
Identification of potential novel therapies
We then matched lists of upregulated genes to drugs that target their gene products. In addition, we obtained lists of multiple targets for each of approximately 2,000 characterized drugs from the literature and online databases.
RESULTS
Model creation, angiography and biopsy
After shunt creation, the animals consistently developed significant PAH in the LPA and survived to 180 days. Aortic and LPA pressures were measured and angiography was performed without complications. The biopsy procedures were safe and effective (Fig. 1). The animals recovered from the catheterization and biopsy procedures well without significant cough, hemoptysis, or respiratory distress. There were no deaths related to the catheterization or biopsy procedures. Single samples from each time point were generally adequate in size for gene expression analysis.
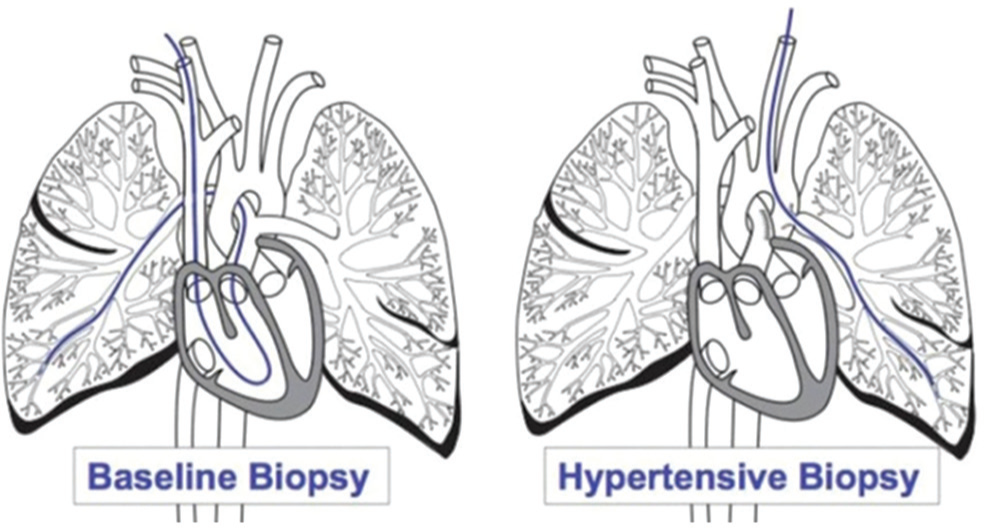
Schematic of biopsy procedures. Baseline biopsy-The catheter is advanced from a jugular vein, through the right heart, into a distal pulmonary artery branch (in this case right lower lobe) to obtain biopsy samples. Hypertensive biopsy- The catheter is advanced from a carotid artery into the aorta and then through the anastomosis into a distal branch of the LPA for biopsy.
Expression analysis
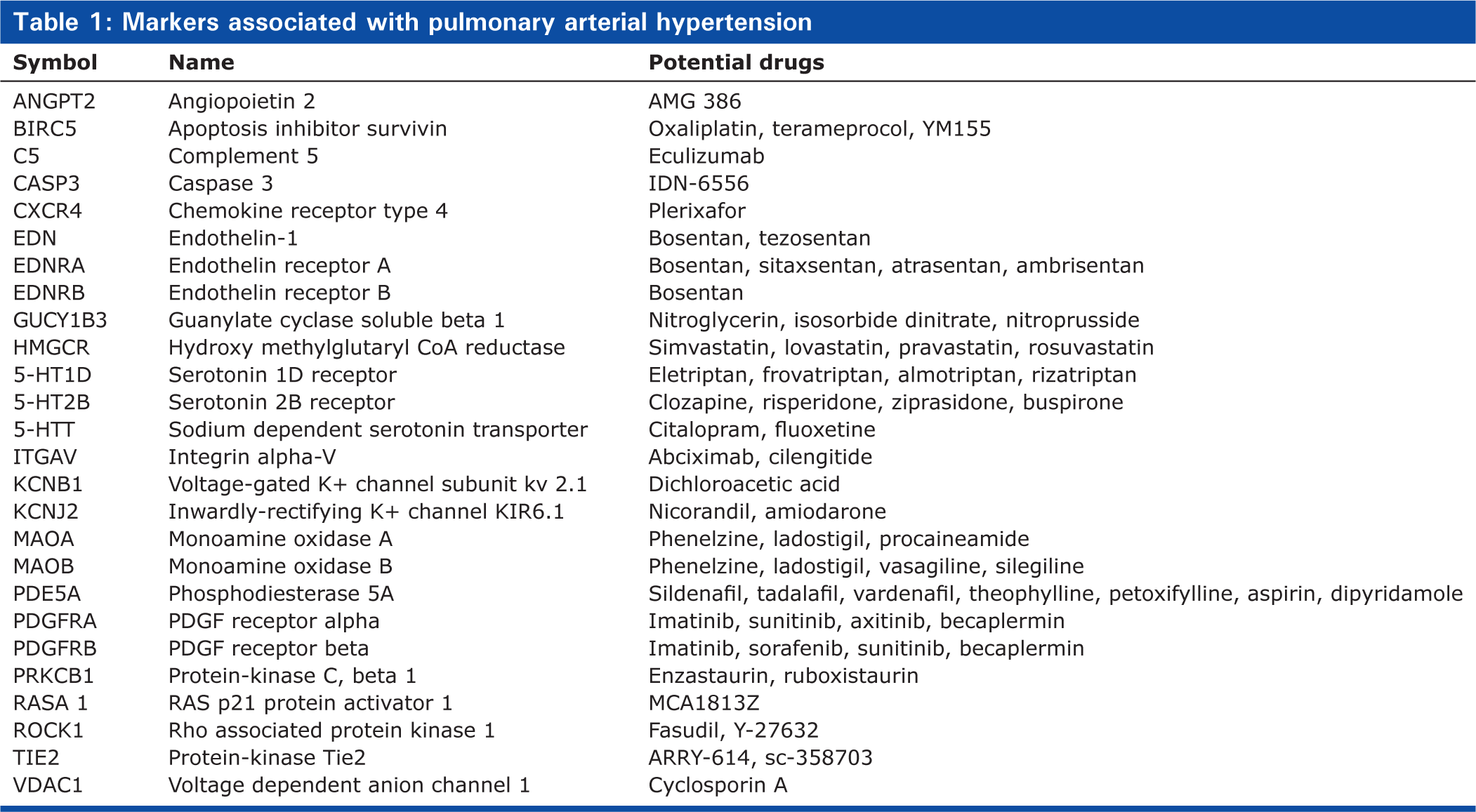
Mean expression values for each gene were obtained by averaging the gene expression values of at least two biopsies at each time point. The resulting gene expression mean values were used to calculate fold changes for Days 7, 60, and 180 relative to baseline in four animals. The validity of the model was confirmed by showing gene expression changes for selected genes previously known to be dysregulated in PAH, including endothelin-1, serotonin 2B receptor and phosphodiesterase 5A, which were upregulated and inducible nitric oxide (NO) synthase, vascular endothelial growth factor beta and inwardly rectifying potassium channels, which were downregulated, in agreement with previous studies.[6] No signal was detected for prostacyclin synthase or BMPR2 in this porcine microarray. Besides changes in genes previously associated with PAH, we observed changes in the expression of many other genes that have not previously been associated with the development of PAH. A selection of these genes is displayed in Tables 1 and 2. Many transcripts increased while many decreased compared to baseline. However, several transcripts showed varying levels at different time-points suggesting the possibility of stage-specific changes in gene expression.
Markers associated with pulmonary arterial hypertension
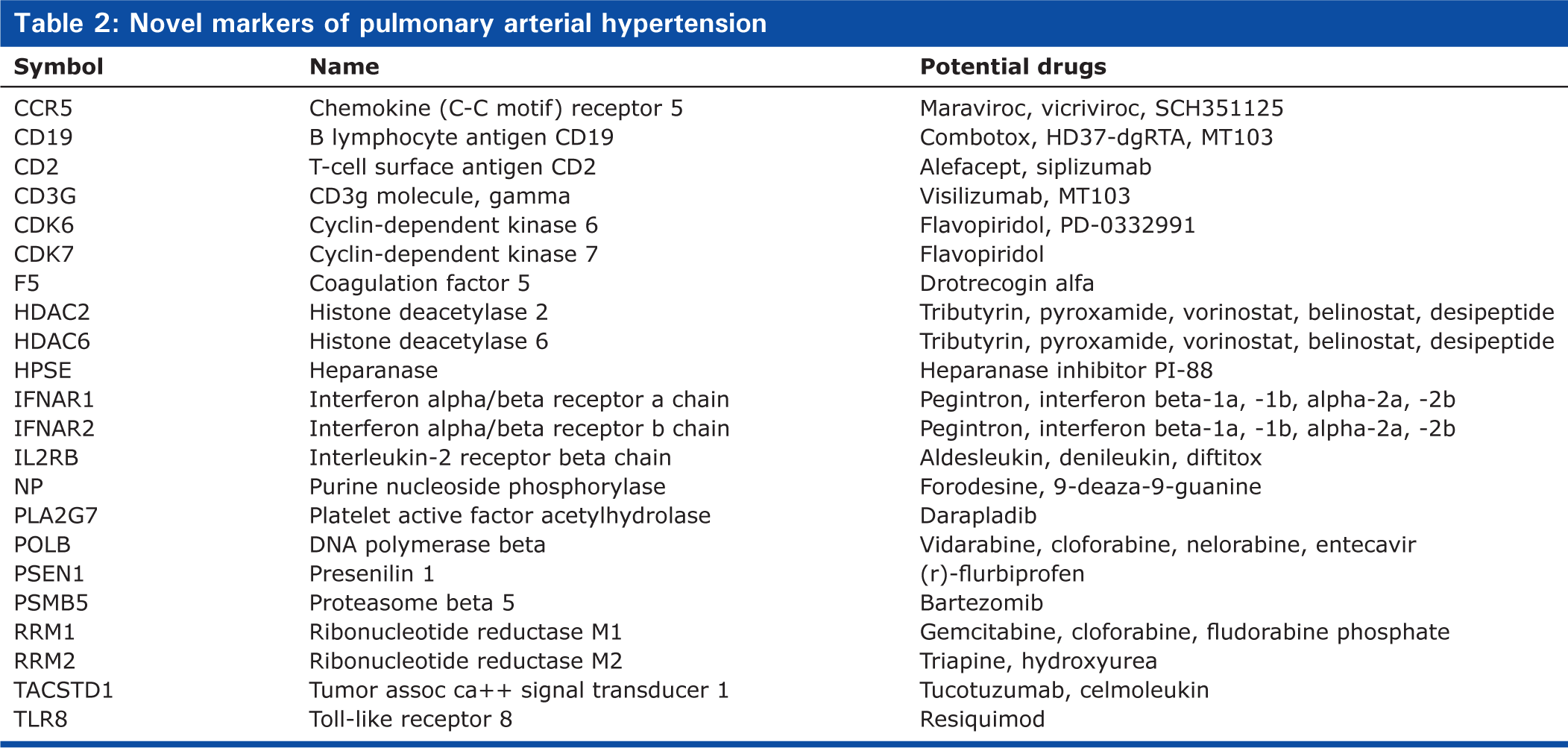
Novel markers of pulmonary arterial hypertension
Baseline
The mean LPA pressure at baseline was 17 mmHg. Angiography and histologic analysis showed normal findings. For purposes of comparison, gene expression at baseline was assigned a level of 1.0 (Fig. 2).
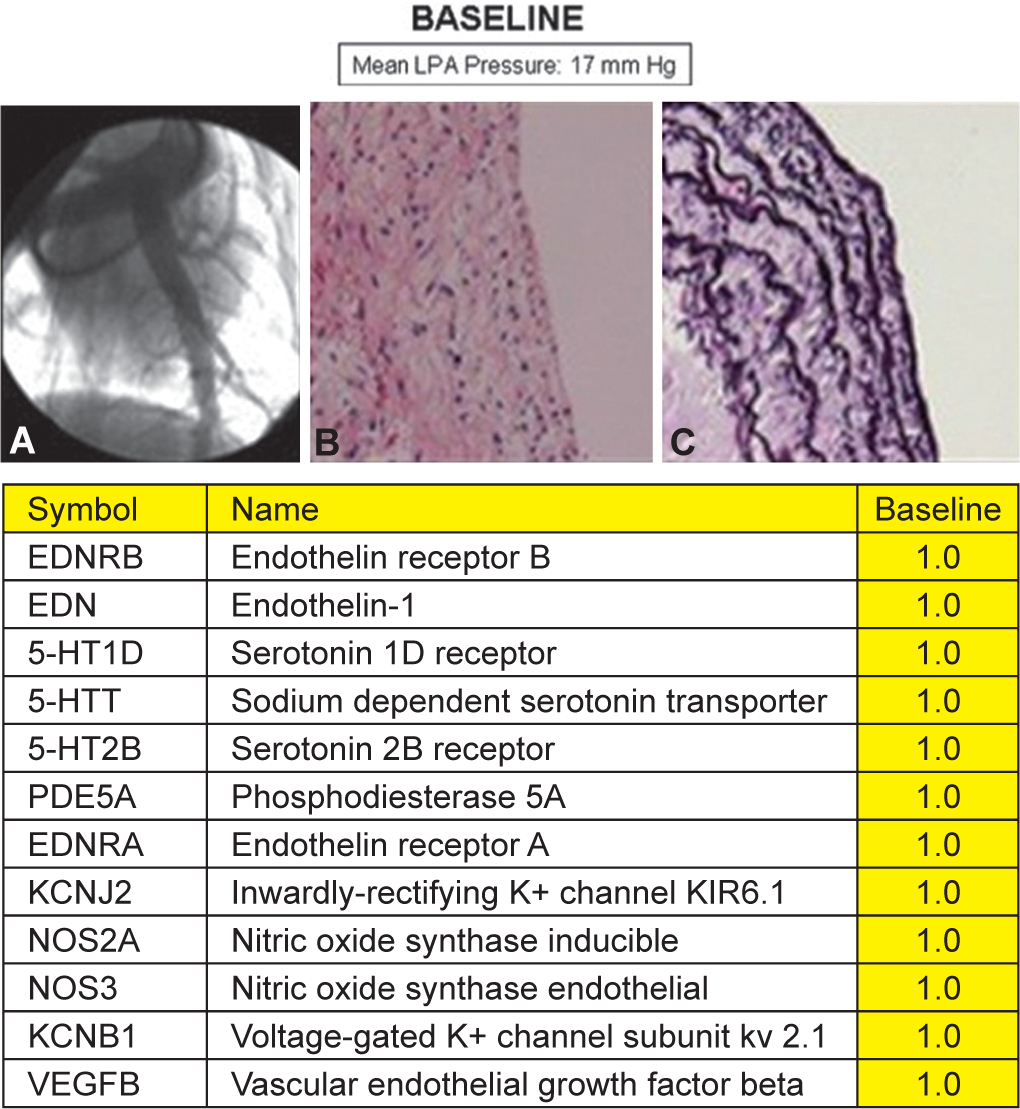
Baseline. Representative angiogram
Day 7
The mean LPA pressure on Day 7 was 34 mmHg. Angiograms showed normal appearing pulmonary arteries. Biopsy samples demonstrated normal appearing histology, except for very mild thickening of the neointima. Several genes showed significant changes in expression (Fig. 3).
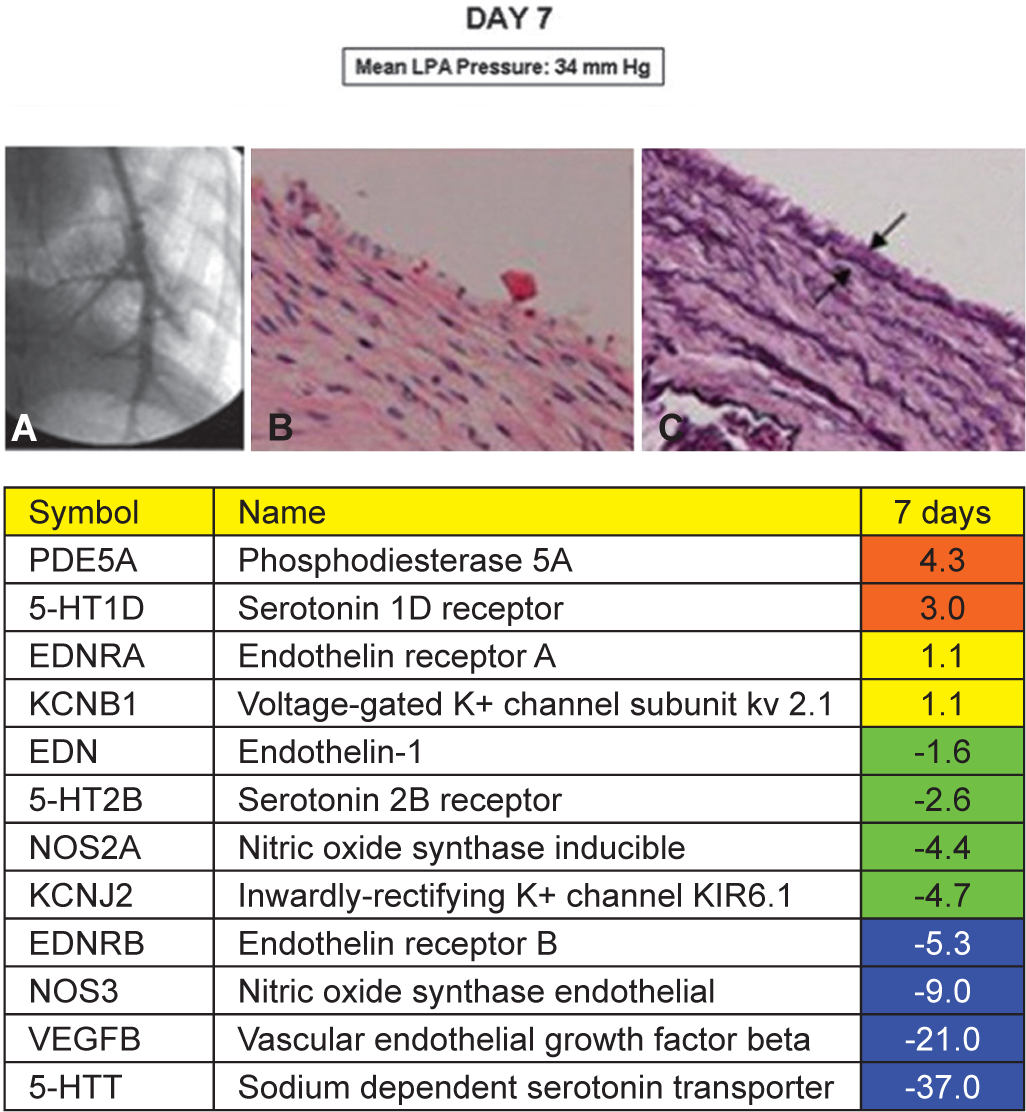
Day 7. Representative angiogram
Days 60 and 180
The mean LPA pressure on Days 60 and 180 was at systemic level (56 to 63 mmHg). Angiograms showed dilation of proximal vessels, tortuosity, irregularities, narrowing and loss of distal arteries and occasional thrombi that were partially or completely occlusive of arterial branches. Histologic examination of biopsy samples from hypertensive pulmonary arteries and lung parenchyma at the time of necropsy showed findings consistent with pulmonary vascular disease, including neointimal thickening, medial hypertrophy, disorganized elastic laminae, myxoid degenerative changes (Figures 4 and 5) and obstructive arterial lesions.[7]
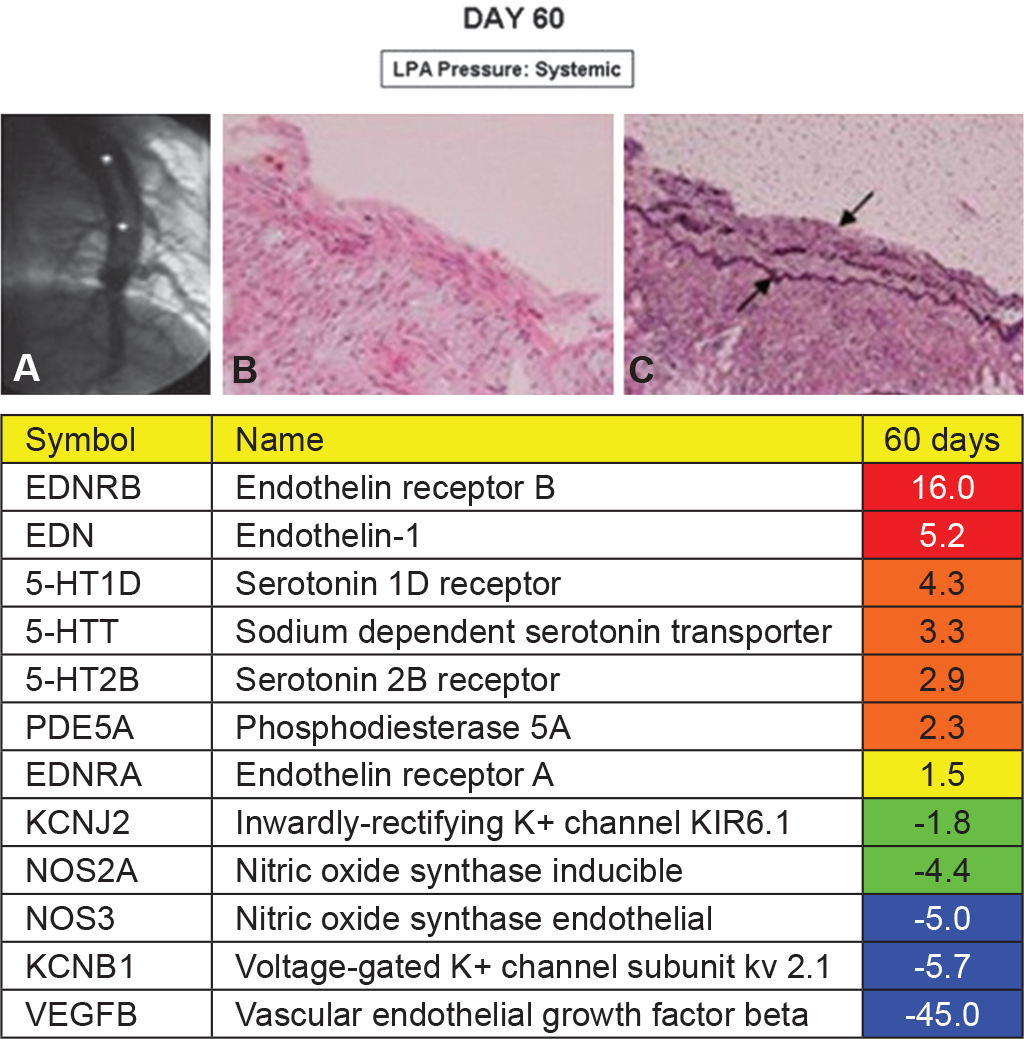
Day 60. Representative angiogram
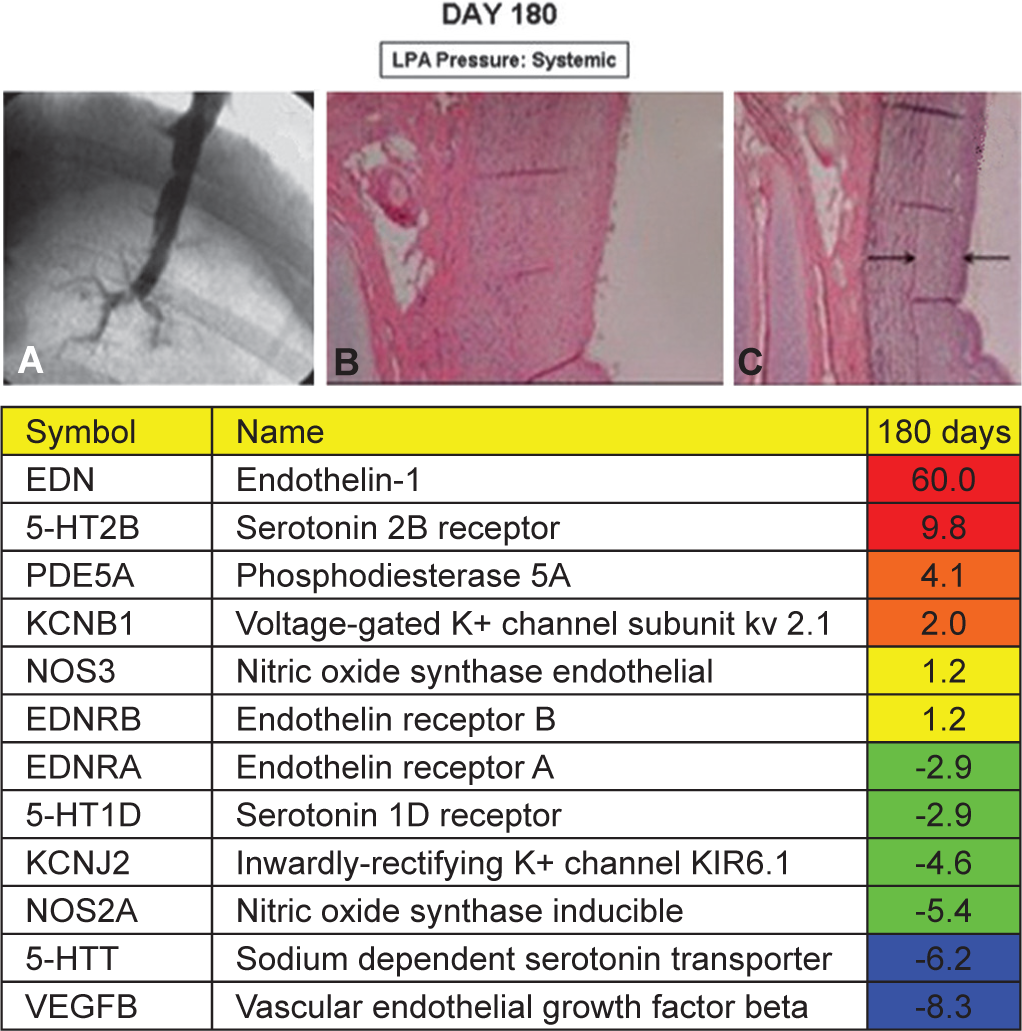
Day 180. Representative angiogram
Gene expression pathways
The gene expression changes relative to baseline were analyzed using Ingenuity Pathway Analysis software and pathway networks were generated. Figure 6 shows an example of a pathway network composed of several genes known to be associated with PAH and potential targets of three sample drugs at Day 60. Similar pathways could be generated for other genes and other time points.
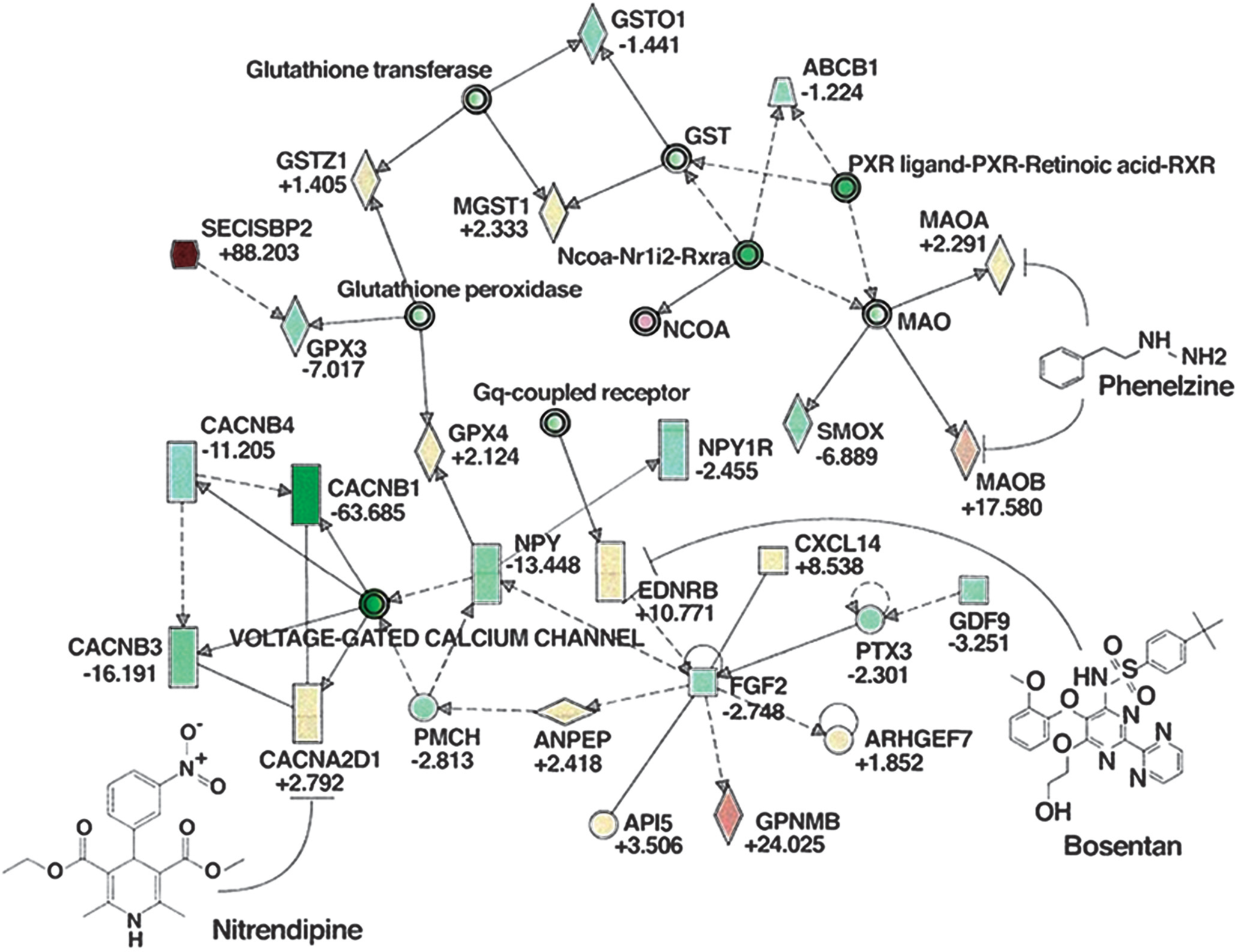
Sample molecular pathway network. EDNRB (endothelin receptor B) molecular pathway network for day 60 constructed using Ingenuity Pathway Analysis shows genes with increased expression (red) and decreased expression (green) (color intensity proportional to fold change; fold changes at day 60 relative to baseline listed underneath each gene symbol) and the targets of three potential drugs: Bosentan (endothelin receptor antagonist), nitrendipine (calcium channel blocker) and phenelzine (dual monoamine oxidase A and B inhibitor).
Pharmacologic targeting
We examined changes in expression for gene targets of many drugs that are currently in use or under investigation for PAH (Table 1). We also identified existing drugs (used in disease processes other than PAH) that target upregulated genes in our model but that have previously not been associated with PAH (Table 2).
DISCUSSION
Percutaneous pulmonary endoarterial biopsy coupled with histologic and molecular analysis represents a potential new paradigm for diagnosis and potential treatment of PAH. Histomolecular analysis could become a routine component of the diagnostic information obtained in patients with pulmonar vascular diseases at the time of cardiac catheterization. In addition to obtaining pressures, cardiac output, calculation of pulmonary vascular resistance, angiography and vasodilator testing, endoarterial biopsy with histologic and molecular analysis would add a whole new dimension of biologic information to aid in diagnosis and choice of therapy. Extensive preclinical experience with endoarterial biopsy suggests that this technique could be tested in the clinical setting.
We chose a chronic swine surgical shunt model[10] because it results in severe PAH, it mimics systemic-to-pulmonary arterial shunts in humans and allows the performance of sequential catheterization and biopsy procedures. Our swine animal model is similar to the one described by Corno et al.[10] However, we modified the size of the anastomosis between the LPA and the descending aorta (4.5 mm) and the size (20-25 kg) and type (Micro) of swine. In our model, the LPA pressure ranged from normal to about half-systemic level seven days after surgery. At Days 60 and 180, the LPA pressure was at systemic level. Angiography at Day 7 showed normal vessels. Angiography at Days 60 and 180 confirmed findings seen in clinical PAH, including dilatation of central arteries, tortuosity, stenosis and loss of distal vessels and formation of partially or totally occlusive thrombi.
Unique to this study was the use of an experimental endoarterial biopsy catheter, which allowed pulmonary vascular biopsy procedures to be performed sequentially as the PAH model developed. The catheter was safe and effective. Vascular changes, including spasm, thrombosis and vessel irregularities were rare, did not cause significant hemodynamic effects and resolved on follow-up angiography. Biopsy samples were adequate for histology. The hypertensive samples showed progressive thickening of the neointima, composed of connective tissue and a few smooth muscle cells and degenerative changes and disorganized elastic laminae in the media. We have previously shown that biopsy samples were also adequate for smooth muscle and endothelial cell culture.[8] In addition, in an experimental model of lung transplantation, we demonstrated that biopsy samples were adequate for PCR analysis and that changes in VCAM-1 mRNA were observed earlier than histologic changes of lung transplant rejection.[11] Including procedures in this study, we have used the biopsy catheter safely and effectively in more than 1,000 experimental pulmonary arterial biopsy attempts.
Transcriptional profiling may allow a better understanding of disease causation, prognosis and therapy. This approach has been applied successfully in patients with cancer and cardiovascular diseases such as cardiomyopathy, heart failure and myocarditis.[12–16] Transcriptional signatures in patients with PAH may help elucidate mechanisms of disease, offer prognostic information and aid in the formulation of disease or stage-specific therapies.
Other investigators have performed microarray analysis in human PAH, including studies of whole lung tissue specimens,[17,18] cells cultured from lungs of patients with PAH,[19] and circulating cells.[20,21] Microarray studies have also been performed in several animal models of PAH, including a porcine model of left lower lobe pulmonary hypertension,[22] genetically modified mice and the effects of pharmacologic agents on mice and rats with PAH.[23,24] These studies showed induction of genes very similar to those observed in human PAH.[25]
In our model, many transcripts changed from baseline through the development of PAH. Several genes known to be dysregulated in PAH were also dysregulated in biopsy samples obtained in our model. These included endothelin-1, phosphodiesterase 5A, rho associated protein kinase 1 and serotonin 2B receptor, which were upregulated. Nitric oxide synthase, calmodulin, inwardly-rectifying K+ channel and vascular endothelial receptor beta, were all downregulated. Others, such as platelet-derived growth factor receptors, endothelin receptors and serotonin 1D receptor, showed variation at different time-points, suggesting a possible stage-specific regulation. The time-dependent variation of gene expression in our model suggests that endoarterial biopsy may detect disease progression-dependent or therapy-induced variations in gene expression in clinical PAH, enabling the design of more personalized therapeutic regimens.
Another important finding in this study was that several genes that displayed the largest changes in expression from baseline were genes associated with inflammation or immune modulation. These include complement 5, T-cell surface antigen CD2, B-cell surface antigen CD19, chemokine receptors 4 and 5 and toll-like receptor 8. Other investigators have also reported an important role of inflammation in PAH[26,27] and the use of anti-inflammatory drugs to treat PAH.[28,29] Inflammation and immune modulation merit further investigation in PAH.
As in this study, the methodology of obtaining histomolecular information from pulmonary endoarterial biopsy could be used in shunt-induced human PAH and other pulmonary vascular disorders such as thromboembolic disease, the diagnosis of lung transplant rejection and pulmonary hypertension associated with other conditions such as high altitude, anorexigen use, infectious etiologies and lung parenchymal diseases. Additionally, the technique could be utilized in diseases affecting other vascular beds.
An alternative explanation for the time-related variation in gene expression in our model may have been secondary to the cell type distribution in the biopsy samples. As shown histologically, biopsies from arteries obtained early during the progression of PAH consisted mostly of medial smooth muscle cells and rare neointimal cells. Biopsies obtained later in the progression of PAH had a higher proportion of neointimal cells. While the majority of neointimal cells are smooth muscle cells, their gene expression profile may differ because their origin could be from the media, the adventitia, or from circulating precursor cells.[30] Nonetheless, the mRNA levels in the biopsy samples provide an in vivo profile of the genetic expression in the vascular wall, which determines the pathophysiology and identifies potential targets for therapy.
From our model, we used the changes in gene expression to identify drugs that could target these genetic changes. Among these are several drugs which are currently approved for use in human PAH or are in experimental trials including endothelin receptor blockers, phosphodiesterase 5 inhibitors and rho kinase inhibitors. Several of the drugs are being tested in animal models. In addition, drugs that have been used in diseases other than PAH, but which also target several transcripts that were dysregulated in our model, offer additional therapeutic options. Finally, the discovery of novel dysregulated mRNAs using this technique opens the door to the development of novel drugs.
This study has several potential limitations. Animal models may not accurately reflect the disease process or progression of human PAH. However, even if the transcriptional profile differed in this swine model and patients with PAH, the technique of obtaining and analyzing pulmonary arterial gene expression could prove useful in disease staging and therapy design. Another limitation may be that biopsies were obtained from vessels ranging in diameter from 1–3 mm and it is unclear whether the gene expression changes in these vessels are representative of changes in the rest of the vasculature. However, changes in these vessels may still be important for disease characterization and therapy. Additional limitations are that the microarray data was not confirmed by PCR analysis and that mRNA levels may not directly reflect the corresponding protein levels in the vascular wall. However, endoarterial biopsy sampling offers a method to compare transcript and protein levels, add to the knowledge of translation and post-translation modifications and identify novel protein therapeutic targets in PAH. Finally, none of the drugs in the lists have yet been fully tested in our porcine model; therefore, their utility remains unproven.
In summary, we describe a new paradigm for endovascular histomolecular analysis in PAH. This technique could improve our understanding of the mechanisms associated with experimental and clinical PAH, elucidate transcript signatures predictive of prognosis, identify novel drug targets and detect stage- and disease-specific variations in gene expression, leading to personalized PAH therapies.