
Abstract
The aim of our study is to determine characteristics and outcomes of kidney cancer in renal transplant recipients. MEDLINE® database was searched in June 2015 to identify cases of kidney cancer in renal transplant recipients. We include also a new case. Descriptive statistics were used for analysis. Forty-eight (48) recipients reported in 25 papers met the eligibility criteria. The median age was 47 years (range 9-66); 27% were females. Chronic glomerulonephritis, cystic kidney disease and hypertension were common indications for renal transplant. Among donors 24% were females and the median age was 52.5 years (17-73); 62% of kidney cancers were donor-derived. The median interval between transplant and cancer diagnosis was shorter for cancer of recipient versus donor origin (150 vs. 210 days). Clear cell carcinoma was diagnosed in 17%. 25% had metastasis at diagnosis. Kidney explantation or excision was done in 90% and 84% of cases with and without metastasis respectively. The median survival was 72 months. Actuarial 1-year and 5-year survival rates were 73.4% and 55.1% respectively. Among the recipients from 7 donors who subsequently developed malignancy, 57% were dead within a year. Kidney transplant recipients have a small risk of kidney cancer, which affects younger patients and occurs within a year of transplant, likely due to immunosuppression. Whether the use of older donors may increase the likelihood needs further investigation. The presence of metastasis, explantation or excision of affected kidney and development of cancer in donors predict outcomes. The results may guide patient education and informed decision-making.
Introduction
Transmission of malignancy from organ donor to recipient, well-recognized complication of transplantation, 1 is rare but frequently unavoidable. 2 About 17,000 of kidney transplants are performed in the US yearly and malignancy is the second most common cause of death (after cardiovascular events and infection) in these cases. 3 In patients with transplants, the incidence of kidney cancer is estimated to be approximately 5%; 10% of these kidney cancers arise in renal grafts.4,5 The rarity of kidney cancers in kidney transplant recipients precludes understanding of the demographics, characteristics, treatment methods and outcomes of this entity. Most of these cancers are treated with explantation or excision of the graft. Chemotherapy and radiotherapy are used mostly as an adjunct. Here we present a case which was treated with explantation, followed by radiation therapy for recurrent disease. We have also reviewed cases of renal malignancy in renal transplant recipients.
Materials and Methods
A systematic search of MEDLINE database (via PubMed) was conducted in July 2015 to identify articles describing a new diagnosis of kidney cancer following kidney transplant. The following terms were utilized for selecting the articles: (Kidney Transplantation OR Renal Transplantation OR Organ Transplantation) AND (malignant OR cancer OR tumor) AND (transmission). The bibliography of each article was hand-searched for additional reports. Only reports published in English language were included. Of a total of 420 searches, 24 articles met the eligibility criteria (Figure 1). Additionally, we also describe an original case report.
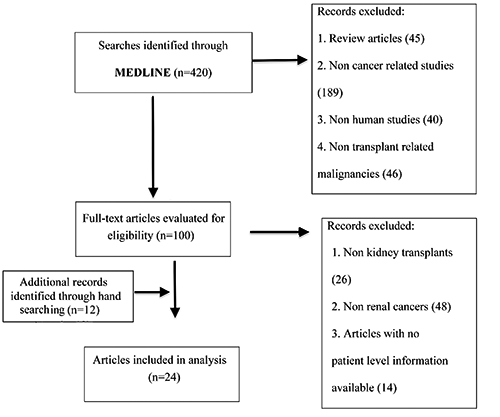
Flow diagram for selection of the articles.
During analysis, details of the patient, transplant history, diagnosis of kidney cancer, therapy, complications and outcomes were obtained until the last follow-up of the patient.
Results
A 55-year-old male presented to emergency department complaining of abdominal pain, distention, as well as nausea and vomiting of 2 days’ duration. He had a bilateral kidney transplant one year ago for end stage renal disease secondary to chronic hypertension. His post-transplant course was complicated by ureteral strictures, enterocutaneous fistula and recurrent small bowel obstructions. The patient was on mycophenolate mofetil, prednisone and tacrolimus to avoid graft rejection. He had a history of heavy smoking, alcohol consumption and cocaine use, but had quit one year ago. Physical examination revealed heart rate of 109 beats/min, blood pressure of 134/96 mm Hg, respiratory rate of 20/min and temperature of 36.6°C. On abdominal examination, there was diffuse tenderness and high-pitched bowel sounds. Rest of the examination was normal.
Laboratory studies included white blood cell count of 10,200/μL with 78% granulocytes, hemoglobin of 16.6 g/dL and platelet count of 155,000/μL. He had a creatinine of 1.04 mg/dL, blood urea nitrogen of 13 mg/dL, sodium of 138 mmol/L, potassium of 3.3 mmol/L, and chloride of 100 mmol/L. Ultrasonography (USG) of right kidney demonstrated a transplanted kidney with a heterogeneous hyperechoic mass measuring 5.5*4.9X5.6 cm. Computed tomography (CT) scan of abdomen revealed right lower quadrant transplanted kidney with a new complex enhancing mass involving the lower pole measuring 5.4×73×6.5 cm, which was highly concerning for malignancy. CT scan also demonstrated new gastric distention, dilated loops of small bowel, fecal material in distal small bowel loops, and air and stool throughout colon, which was concerning for small bowel obstruction. Whole body positron emission tomography (PET) scan depicted a 73×6.4×6.2 cm inferior pole mass within right lower quadrant kidney transplant with a maximum SUV of 9.6, suspicious for primary renal cell carcinoma versus lymphoma. Biopsy of the mass showed sarcomatoid carcinoma with squamous differentiation, possibly of the uroepithelial origin.
The patient underwent nephrectomy of the right transplanted kidney. Pathology revealed high-grade carcinoma with squamous differentiation and sarcomatoid areas (sarcomatoid carcinoma/carcinosarcoma) with a tumor size of 6.7 cm in the greatest dimension. Tumor appeared to be arising in the setting of keratinizing squamous metaplasia involving the right renal pelvis and calyceal system with invasion into renal parenchyma and peripelvic adipose tissue (pT3). Margins were positive in areas where capsule was stripped but there was no lymphovascular invasion. Periureteral tissue was also involved with invasive carcinoma with squamous differentiation. Cytogenetics report showed: 68-77, XXY,+1, add (1)(p11),i(1)(p10)x2,-3,+6, add(7)(p15),add(7)(p21),add(7)(q32), add(8)(p22),-9, i(9)(q10)x2,add(11)(q14),-13,-13,add(16)(q24), add(17)(p13),+add (19)(q133),+21,add(21)(p11.1)x2,-22,+7-12 mar, 0-3dmin[cp 17]/129, slx2[1]//46, XX[2].
A repeat PET/CT scan in a month revealed 2.1×53 cm soft tissue fullness in the right pelvis at the site of prior mass resection/nephrectomy. This lesion was markedly hypermetabolic with maximum standardized uptake value (SUV) of 13.0 compatible with recurrent local malignancy. Retroperitoneal and inguinal lymph nodes were not enlarged or PET-avid. The patient refused chemotherapy and therefore, was treated with a course of radiotherapy to 4230 cGy in 16 fractions. A follow-up PET scan showed a 1.9×1.7 cm minimally hyper metabolic focus of activity in the right pelvis with a SUV of 3.6. At 18 months’ follow-up, the patient is alive without any recurrence of cancer.
Review of Reported Cases
A total of 48 patients reported in 25 articles (along with our case report) met the eligibility criteria (Table 1). The median age of recipients was 47 years (range 9-66), and 27% were females. The cause for renal transplant were: chronic glomerulonephritis (22%, n=6),6–10 polycystic kidney disease (11%, n=3),8,11,12 hypertension (11%, n=3),13,14 IgA nephropathy (8%, n=2), 10 renal pelvis carcinoma with left nephrectomy (4%, n=1), 15 nephronopthisis (4%, n=1), 16 congenital nephrotic syndrome (4%, n=1), 10 amyloid disease (4%, n=1), 17 diabetes mellitus (4%, n=1), 6 interstitial nephritis (4%, n=1), 18 Henoch-Schonlen purpura (4%, n=1), 19 Alport syndrome (4%, n=1), 18 neurogenic bladder (4%, n=1), obstructive uropathy (4%, n=1) and ESRD of unknown origin (8%, n=2).20,21
Kidney cancer in recipients of kidney transplant.
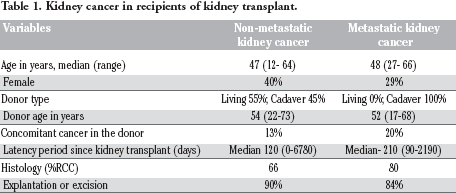
The median age of donors was 52.5 years (range 17-73) with 24% of them being females. Where data was available, 60% (n=22) of the donors were cadaver,6–8,12–15,17,18,21–28 while the rest (n=15, 40%) were living.2,11,16,19,20,28,29 Six of the living donors were related to the recipients.16,19,20,28,29
Seven donors were subsequently found to have malignancy including clear cell carcinoma,
20
hypernephroma,
11
anaplastic tumor on nephrostomy scar,
29
metastatic adenocarcinoma with unknown primary,
13
primary hepatocellular carcinoma,
9
metastatic giant and spindle cell carcinoma of thyroid,
15
and a lung tumor.
30
Out of seven, 2 donors were diagnosed with malignancy after 8 months and 10 months of transplantation.28,29 One donor had a renal cyst which was excised during the transplantation, and subsequently found to be a renal cell carcinoma.
20
Three donors had history of malignancy in other organs with no identified metastasis to kidney at the time of donation.9,13,15 Tunner
The median time interval from transplantation to presentation or diagnosis of the malignancy in recipients was 210 days. The latency period between transplant and cancer diagnosis was 272 days in cancer of recipient origin in comparison to 210 days in those with cancer of donor origin.
Biopsy was done for the diagnosis of cancer in 100% (n=48) of recipients, and 69% (n=33) of the cancers had RCC. The most common type of RCC was clear cell carcinoma (27%, n=9)7,10,12–14,20,21,31 while the other types were: sarcomatoid (15%, n=5),2,8 angiosarcoma (6%, n=2), 18 renal papillary tumor (6%, n=2),28,31 anaplastic (6%, n=2),25,29 chromophobe (3%, n=1), 16 cystic adenocarcinoma (3%, n=1), 31 anaplastic adenocarcinoma (3%, n=1), 29 giant and spindle cell carcinoma (3%, n=1), 15 and undifferentiated (6%, n=2).17,22 The type of renal cell carcinoma was not mentioned in the rest (22%, n=7),2,6,19,31 Other tumors (31%, n=15) comprised 31% of the cases which included: undifferentiated cancer (20%, n=3), 6 invasive urothelial carcinoma (7%, n=1), 24 papillary transitional cell carcinoma of bladder (7%, n=1). 31 Thirty-three percent of the tumors were subsequently found to be benign and the type of cancer was not mentioned in the rest (33%, n=5).
Fifty-five percent (n=31) of the tumors were donor in origin, while 39% (n=22) originated from the recipient. The rest (6%, n=3) were determined to be derived from both donor and recipient. For example, one of the tumors in Pedotti
Explantation of the graft or excision of the tumor or a part of the graft, and discontinuation of immunosuppressants along with supportive treatment were used for management in most cases. Explantation or excision was done in 90% of the nonmetastatic malignancies, while 84% of metastatic malignancies underwent explantation or excision. Chemotherapy,6,7,12,24,28 radiotherapy,13,18,29 or both 18 were also used in 9 cases. While 64% (n=7) of the 9 cases had metastasis,7,12,13,17,18,24,32 18% (n=2), 29 had no metastasis, and the status of metastasis was not mentioned in the rest, (18%, n=2). 6 In one case treated with local irradiation, distant metastasis was diagnosed at autopsy. 29 Local irradiation was administered to treat recurrent local malignancy in our case after initial explantation.
The median survival was estimated to be approximately 72 months. Actuarial 1-year and 5-year survival rates were 73.4% and 55.1% respectively. Out of eleven recipients, who died after transplant, 9 were due to malignancy-related causes,6,8,11,15,17,18,24,26,29 while 2 were due to other causes.
2
The recipient in Llamas
Discussion
Our review revealed post renal transplant malignancy in a total of 48 recipients. RCC, the most common type of kidney cancer in adults, was diagnosed in the majority of our cases. Twenty-seven percent of the renal cell carcinoma were clear cell carcinoma which is the most common RCC type. RCC is also known to be the most frequently reported non-central nervous system (CNS) tumor transmitted by transplantation, followed by melanoma and choriocarcinoma. 33 Twelve percent of the cases in our review, including our case, had a sarcomatoid differentiation. The incidence of tumors with sarcomatoid differentiation in general population is estimated as 1-8%, although as high as 32% has been reported.34–37
In our review, the median age of recipients at diagnosis was 49 years while the median age of donors was 52.5 years. The median age at diagnosis for RCC is 64 in normal population, and is unusual in patients under 40 years of age and rare in children.38–40 Immunosuppression in recipients may be one of the factors behind the development of malignancy at an early age. In addition, RCC may also occur in children receiving renal allografts from adults. 16
Chronic glomerulonephritis, hypertension and cystic diseases of kidney were the common factors leading to end stage renal disease in our review. Our case also had a history of chronic hypertension and heavy smoking. In fact, hypertension, smoking, obesity and polycystic kidney disease have been well-recognized risk factors for the development of RCC in normal adults.41–45
The malignancy in post-transplant cases might be due to
Different factors such as type, level and extent of immunosuppression, the use of drugs such as cyclosporine and azathioprine, carcinogenic factors such as sun exposure, genetic predisposition to cancer, pretransplantation dialysis, and the presence of particular viral infections are associated with development of
The outcome for transplant recipients with neoplastic complications is unclear. We calculated the median survival to be 72 months. Actuarial 1-year and 5-year survival rates were 73.4% and 55.1% respectively. In our review, 25% of deaths were related to malignancy. In a review of data from different sources by Briggs
Conclusions
Kidney transplant recipients have a small but definite risk of kidney cancer. It affects younger patients and usually occurs within a year of transplant, likely due to immunosuppression. Whether the use of older donors may increase the likelihood needs further investigation. Explantation or excision of the graft is the most important treatment for localized disease, while radiotherapy and chemotherapy may be used as adjunct in select cases. The presence of metastasis, explantation or excision of affected kidney and development of cancer in donors may predict outcomes. The results may guide patient education and informed decision-making.
Footnotes
Acknowledgement
Vijaya Bhatt is supported by the 2015-2016 Physician-Scientist Training Program Grant from the College of Medicine, University of Nebraska Medical Center.