
Abstract
Malignant melanoma, as the name implies, is a malignant tumor of melanocytes, found in the skin, eyes, meningeal lining and the mucosal epithelium of the aero-digestive and genitourinary tracts. Malignant melanoma is typically skin malignancy, which rarely presents at extracutaneous site. Here we present a rare case of primary retroperitoneal melanoma and review the findings in comparison with other cases described in literature.
Introduction
Primary retroperitoneal melanoma (PRM) is an exceptionally rare extracutaneous malignant melanoma. PRM cases are mostly incidental finding. Only three cases of PRM have been reported in the English literature.1–3
Although malignant melanoma is typically a skin malignancy, it still appears in other organs, where melanocytes can be found (eyes, meninges and the lining of aero digestive tracts).4,5 Atypical extracutaneous melanomas are either metastatic melanoma of unknown primary or very rarely, primary melanoma. Primary extracutaneous melanoma constitutes 4-5% of melanoma cases.4–6
Case Report
A 53-year-old Caucasian female, with no significant comorbidities except for well-controlled hypertension and hypothyroidism, presented with postmenopausal vaginal bleeding. Transvaginal ultrasound revealed left side complex pelvic mass measuring 4.3×3.4×3 cm, with differential diagnosis of either complex cystic or solid adnexal mass. So, laparoscopic hysterectomy and bilateral salpingo-oophorectomy was performed along with removal of left pelvic mass, pelvic lymph node dissection and omentectomy. She tolerated the procedure well and was discharged shortly thereafter. Gross examination of the pelvic mass showed a fatty nodule measuring 7.3×5.5×3.3 cm and weighing 78 g (Figure 1A). The serial sectioning revealed tan-white to red-brown cut surfaces (Figure 1B). Histopathological examination showed neoplastic proliferation of spindled cells with ovoid vesicular chromatin, visible nucleoli, indistinct cell borders, apoptosis, geographic necrosis and mitoses. There were scattered clusters of pigment-laden histiocytes with very dark pigment material. Lymphocytes were seen scattered throughout the tumor (Figure 2). Immunohistochemical (IHC) staining was done with appropriately staining controls and showed the following results; HMB45: Positive, Melan-A: Positive, S100: Positive and Cytokeratin: Negative (Figure 3). No other pathology was identified among other parts including pelvic lymph nodes.

A) Gross pathology of pelvic mass. Whole pelvic mass, post-formalin fixation, inked black and serially sectioned, showing fleshy, variegated gray-tan and gray-white cut surfaces; B) gross pathology of pelvic mass. Slice of tumor near one end showing discrete, black, lobulated sub capsular area at top right.
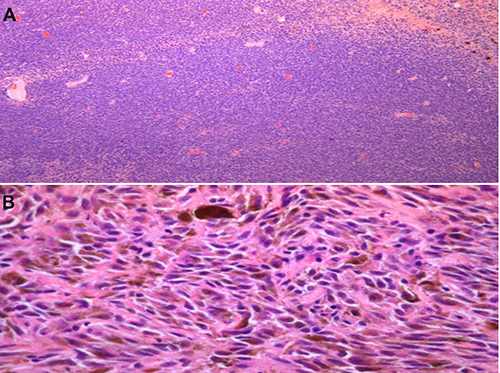
A) Hematoxylin-eosin (H&E) slides: spindled cells and ovoid cells comprising the hypercellular tumor; B) H&E slides: tumor cells with melanin pigment (brown).

A) Immunostaining with HMB45 (+melanocytes); B) immunostaining with Melan-A (+melanocytes); C) immunostaining with S100 (+melanocytes).
The histomorphological features and IHC staining pattern were most consistent with the diagnosis of a malignant melanoma. Given the pelvic retroperitoneal location of the mass, this was thought to be a metastatic deposit.
Due to the rarity of her presentation and lack of evidence based guidelines for further work up, an extensive work up was performed to search for an occult primary and involvement of other sites. Detailed skin examination, positron emission tomography - computed tomography scan, magnetic resonance imaging brain, colonoscopy and esophagealgastro-duodenoscopy did not reveal any abnormalities. Further pathology studies did not reveal BRAF or C-Kit mutation. Hence, diagnosis of primary retroperitoneal melanoma was made. The patient was offered adjuvant immunotherapy (interferon) as in high risk cutaneous melanoma; however, she opted for observation after considering the treatment toxicities and survival data.
Discussion
Very few cases of PRM have been reported in medical literature.1–3 Due to its unusual location, the diagnosis of extracutaneous malignant melanomas is a challenge. In fact, it is more difficult to diagnose PRM because the retroperitoneum does not contain melanocytes. The large space of the retroperitoneal cavity provides ample room for the solid tumors to grow without being noticed, and thus it rarely remains the only site of disease.
Due to rarity of PRM there is no established recommendation for diagnostic workup and therapeutic options.
The diagnosis of PRM is possible only after histopathological examination and IHC studies. However, histopathology cannot determine whether melanoma presenting retroperitoneal mass is PRM or metastasis from cutaneous or visceral melanoma. In 1976, Ainsworth and colleagues 7 and, subsequently, in 1984, Carstens and colleagues 8 established a series of criteria to distinguish between primary and metastatic malignant melanomas.
Conclusions
The possibility of PRM must be kept in mind while evaluating an unexplained solid retroperitoneal mass and the diagnosis confirmed by IHC. Despite the fact that melanoma can have varied presentations, PRM is still a very rare entity among extra cutaneous malignant melanomas.
This case has been highlighted for its rarity and unusual presentation and must be included among the few reported cases of PRM.
Footnotes
Acknowledgments
The authors would like to thank Teresa Limjoco, MD. Clinical pathologist for slides supplement.