
Abstract
Carcinoma ex pleomorphic adenoma (CXPA) is exceedingly rare in minor salivary glands of oral cavity. We present a case of CXPA arising from buccal mucosa in a 44-year-old male patient. The man presented to surgery outpatient department with right buccal mucosa swelling. Clinical impression suggests a neoplasm of buccal mucosa and the patient was sent for fine needle aspiration cytology. By examining the cytological smears, possibility of carcinoma was revealed. The mass was dissected and excised with safety margins. Examining Hematoxylin and Eosin slides, final diagnosis of CXPA was given. Patient did not turn for regular follow-ups and presented 1 year after surgery with recurrence at the same site. CXPA is an uncommon malignant tumor with highly aggressive biological behavior. Its occurrence in sites like buccal mucosa is rare. Hence, quite a diagnostic challenge at such sites cause diagnostic difficulties.
Introduction
Carcinoma ex pleomorphic adenoma (CXPA) is a rare malignant epithelial tumor arising from pre-existing pleomorphic adenoma. It commonly originates in parotid gland. In minor salivary glands, CXPA often occurs in palate, whereas is rare in buccal mucosa. Hereby, we report a case of CXPA of buccal mucosa in a 44-year-old male and present a review of previous literature.
Case Report
A 44-year-old male presented to surgery OPD with right buccal mucosa swelling. He was complaining of swelling since a long time in the past, approximately, for last 8-10 years. Recently for past 1-2 years, there was increase in size of swelling. The swelling was not painful and did not trouble him, but it had become increasingly noticeable. There was no history of trauma. General health status was unremarkable. Physical examination revealed a 2.5×2.5 cm, firm, ill-defined, non-tender mass in right buccal mucosa lateral to upper premolars. The overlying mucosa was unremarkable. There was no indication of trismus, paralysis or any associated lymphadenopathy. Laboratory examination was within normal range. Clinical impression was that of neoplasm of buccal mucosa and patient was sent for fine needle aspiration cytology (FNAC). FNAC was performed intraorally with 22 g needle and aspirated material was smeared on glass slide. The smears were stained with MGG stain and on examining the cytological smears, possibility of carcinoma was suggested. The mass was dissected and excised with safety margins under general anesthesia. The tumor was located immediately beneath the mucosa. It did not involve the facial muscles. On examining H and E slides, final diagnosis of CXPA was given. Patient did not turn for regular follow- ups and presented 1 year after surgery with history of reoccurrence at the same site.
Pathological Findings
Cytological smears were moderately cellular showing tumor cells in cohesive clusters and few singly scattered tumor cells. Tumor cells showed moderate anisopoikilocytosis with high N/C ratio, irregular nuclear contours, conspicuous nucleoli and scant to moderate bluish cytoplasm (Figure 1). Few tumor giant cells were also seen. Background was dirty, necrotic and showed inflammatory cells. Few stromal fragments were also identified in background. Possibility of carcinoma was suggested and excision of mass was advised.

Cytosmears showing tumor cells arranged in acini showing high N/C ratio, irregular nuclear contours, and scanty cytoplasm and inset showing 3-D clusters of tumor cells (MGG, 40×).
Excised specimen was sent for histopathological examination. Grossly, it was grey brown in color measuring 2×1.5×1 cm. cut section showed grey white firm to hard areas with multiple cystic areas. H and E sections showed tumor with features of biphasic pattern consisting of epithelial and mesenchymal components. Majority of areas showed an invasive tumor arranged in nests, ducts, islands, cribriform and acinar pattern (Figure 2). Tumor cells have high N/C ratio, vesicular chromatin, and prominent nucleoli. Intervening areas showed desmoplasia. At places, clearing of tumor cells along with squamoid change was also seen. Areas of capsular infiltration were seen. Final diagnosis of CXPA was rendered.
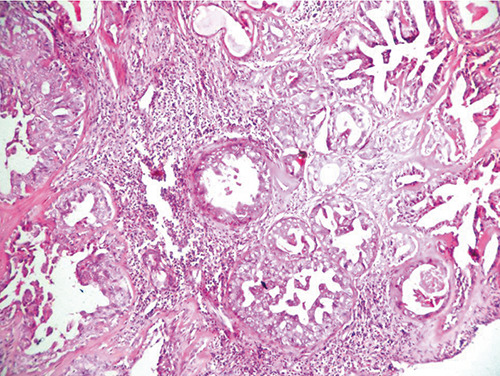
Sections showing an invasive tumor arranged in ducts, acini, cribriform pattern and occasional micropapillary arrangement (Hematoxylin and Eosin, 40×).
Discussion
CXPA is a carcinoma arising from primary or recurrent benign pleomorphic adenoma. 1 CXPAs comprise about 3.6% of all salivary tumors, 6.2% of all mixed tumors, 12% of all salivary malignancies.1,2 Despite that CXPA is uncommon and has a prevalence rate of 5.6 cases per 100,000 malignant neoplasms and yearly incidence of 0.17 tumors per 1 million people. 1 The cancer is found predominantly in 6th to 8th decade and slightly more common in females. 1 The most frequent affected site is parotid gland and submandibular gland is secondary. 3 The cancer is also known to occur in minor salivary glands in oral cavity particularly hard and soft palate.4,5 CXPA from buccal mucosa is extremely rare and only few case reports have been reported.2,3,6 Therefore from point of view of tumor origin, this case seems rare. In addition to these sites, CXPA has also been reported in breast, trachea, lacrimal gland and nasal cavity.7–10 Frequent clinical symptoms include a painless mas but pain, facial nerve palsy, ulcer and swallowing disorder has also been reported. 3 In most cases, CXPA can be asymptomatic as most cancers are not widely invasive and often have similar clinical presentation as PA. The reported duration from onset to diagnosis has been variable from several months to over 20 years. 3 Since presenting symptoms are quite similar to those presenting with benign PA, it is important that clinicians maintain high level of clinical suspicion which can be challenging considering rarity of this cancer and at rare sites, it can manifest like in our case.
CXPA, by definition is composed of mixture of PA and carcinoma on microscopic examination. The proportion of benign versus malignant components can be variable. Based on histopathological examination, CXPA can be sub-classified as i) non invasive ii) minimally invasive (<1.5 mm penetration of malignant component into extracapsular tissue) and, iii) invasive (1.5 mm invasion from tumor capsule to adjacent tissue).11,12 The common malignancies occurring in background of PA are adenocarcinoma NOS (42.4%) and salivary duct carcinoma (32.8%). 13 The other uncommon malignancies that can arise in setting of PA are adenosquamous carcinoma, adenoid cystic carcinoma, undifferentiated carcinoma, myoepithelial carcinoma and sarcomatoid carcinoma. 13 In our case, it was adenocarcinoma NOS developing in setting of PA.
Pre-operative diagnosis of parotid neoplasm is based on history, clinical findings, imaging, and FNA findings. FNAC is commonly used preoperatively to diagnose CXPA. The sensitivity is however low largely related to sampling error, 1 cytomorphological variety and lack of experience. 14 In our case, intraoral FNAC was performed because of bulk of neoplasm towards buccal mucosa. Considering the polymorphic nature of some salivary gland tumor, it is advisable to aspirate more areas to render the correct cytodiagnosis. Aspiration from multiple sites is mandatory in salivary gland lesions clinically suspicious of malignancy. Differential diagnosis of slow growing mass that had recently exhibited a growth spurt should raise suspicion of CXPA. CXPA can be mistaken for PA. It can also be misdiagnosed as other benign and malignant salivary gland tumor. Although occasional cytological atypia may be encountered in same PA, the presence of numerous atypical cells, an abnormal chromatin pattern and necrosis are features important in distinguishing PA from malignant tumors including CXPA. A high grade salivary gland adenocarcinoma that is difficult to classify should include CXPA in its differential diagnosis.
The low sensitivity of FNA may hamper appropriate planning of the extend of surgery. Although, the diagnosis of a non-invasive CXPA would require less aggressive surgery, cytologically it is difficult to almost impossible to distinguish between non-invasive and invasive CXPA. Hence, while the diagnosis of malignancy can be made on FNAC, the extend of infiltration by malignancy may not be possible to discern. 15
Surgery is currently the primary treatment for CXPA. Extend of surgery must be individualized on basis of tumor location and involvement of adjacent structure. For instance, for parotid CXPA total or radical parotidectomy is indicated for frankly invasive CXPA and facial nerve should be resected if directly involved by tumor. However superficial parotidectectomy can be used for some early tumors localized in superficial lobe. Little literature is available for treatment modalities of CXPA at rare sites like buccal mucosa. On average, cancer at these sites tends to be smaller than those arising from major salivary glands. Post-op radiotherapy was usually used for CXPA with advanced stage, high histological grade, node and perineural involvement while surgery alone may be therapy option for small carcinomas.11,16
Conclusions
Carcinoma ex pleomorphic adenoma is a rare neoplasm, seen most commonly in parotid gland. In sites like buccal mucosa, this neoplasm is very infrequent and hence diagnostic challenge for oral pathologists and treating clinicians.