
Abstract
Atypical polypoid adenomyoma (APAM) is a rare polypoid tumor of the uterus composed of atypical endometrial glands surrounded by smooth muscle. A 29-year-old nulligravida, was clinically diagnosed with endocervical myoma and underwent trans-uterine cervical resection with hysteroscope. The histopathological diagnosis of specimens was APAM. Eight months later, she diagnosed recurrent uterine tumor. The positron emission tomography (PET-CT) imaging showed an increased fluorodeoxyglucose uptake. She has performed hysterectomy and was diagnosed APAM. Therapy for APAM depends on multiple factors such as age at presentation and desire for childbearing among others. This is the first report of PET-CT findings in APAM.
Introduction
Atypical polypoid adenomyoma (APAM) is a rare polypoid tumor of the uterus composed of atypical endometrial glands surrounded by smooth muscle. This is classified as a benign mixed epithelial and mesenchymal tumor. 1 Less than 200 cases have been reported about APAM and it most often occurs in young nulliparous women.2–5 Fertility-sparing management for APAM is considered for those who desire pregnancy and can be a cause of female infertility.2–5 It often occurs in reproductive-age women with abnormal genital bleeding. These tumors are often clinically confused with malignant tumors because their cytologic atypia causes tumor cytology results to be positive. Recurrent or persistent lesions after conservative management are common, and coexisting endometrioid adenocarcinoma can be observed in some cases.6–8 There are some reports magnetic resonance image (MRI) findings of APAM. Nonetheless, very few Positron emission tomography (PET-CT) findings of APAM have been reported. To our knowledge, this is the first report of PET-CT findings in APAM. Hence, the purpose of our report is to describe PET-CT findings in a patient with pathologically proven APAM.
Case Report
A 29-year-old nulligravida, not having experienced sexual intercourse Japanese woman, with a body mass index of 25.0 kg/m2 and regular menstrual periods, have Kabuki make-up syndrome with mild mental retardation. According to her family history, her mother was diagnosed with breast cancer at 32 years old, maternal grandfather and uncle were diagnosed with gastric cancer. Our patient was clinically diagnosed with endocervical myoma and underwent trans-uterine cervical resection with hysteroscope (TCR) at the age of 28 years (Figure 1A). The histopathological diagnosis of specimens was APAM with a markedly complex architecture of the glands (Figure 1D). After the procedure, there were no abnormal findings by hysteroscope and ultrasonography. For 8 months later, she visited our clinic with a chief complaint of abnormal uterine bleeding which had shown recurrent uterine mass with bizarre surface same as previous tumor. Transvaginal ultrasonography showed a tumor arising from uterine fundus.

Gross and histologic findings. A) Gross tumor findings. Macroscopic findings (B) pre-fixed and (C) formalin (10%) fixed tissue. Histological findings (D) at first procedure (40×), hysterectomy (E) 40× and (F) 400×. G) Immunohistochemical staining for alpha-smooth muscle actin.
The tumor surface cytology showed atypical glandular cell. MRI findings suggested myometrial invasion of a tumor arising from uterine fundus which includes palisaded low intensity layer (Figure 2A,C) after gadolinium injection. Preoperative staging included a fluorodeoxyglucose (FDG) PET-CT to assess tumor extension and metastatis. The PET-CT acquisition was in 3D-mode, 60 minutes after intravenous injection of 4.5 MBq/kg 18F-FDG. A dual-phase study was also performed on the pelvis 150 min after the injection. The imaging showed an increased FDG uptake; the maximum Standard Uptake Value of corpus uteri was 8.37 kBq/mL and uterine cervix was 11.18 KBq/mL one hour after injection (Figure 2B,D). No other areas demonstrated activity. PET-CT and MRI findingscould not exclude malignancy of the uterine mass. Informed consent for hysterectomy was obtained. Macroscopic examination of hysterectomy specimens showed an exophytic polypoid tumor in the fundus and infiltrative growth in the cervix (Figure 1B,C). Histopathological findings showed that the vast majority of the tumor, including the infiltrative mass in the cervix, was APAM with no malignant foci and squamous morule formation was present in the area of APA. (Figure 1E,F). Immunohistochemical staining for alpha-smooth muscle actin was positive in the myomatous stroma of APAM (Figure 1G). The patient's postoperative outcome was uneventful, and she was discharged on postoperative day 7. No evidence of recurrence and metastasis have found following one year.
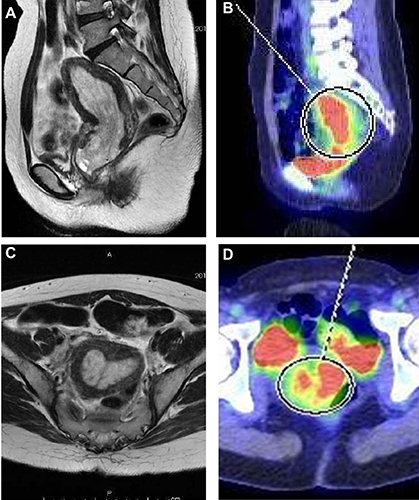
Images of atypical polypoid adenomyoma: A) magnetic resonance imaging (MRI) and B) positron emission tomography-computed tomography (PET-CT) sagittal section, (C) MRI and (D) PET-CT coronal section.
Discussion
APAM is generally benign and mostly occurs in premenopausal women (mean age, 40 years);2–5 therefore, fertility-sparing management should be considered. However, careful follow-up is required because there is a risk of recurrence of APAM or transition to endometrioid adenocarcinoma. This was described as a distinct disease entity by Mazur. 9 Of these patients, 32 (68%) of 47 patients were nulligravida,2,3 86 (70%) of 123 patients were nulliparous,2–5 and clinical histories of infertility are common (29.4-35.3%).3,5 The recurrence of APAM among patients treated with conservative management was 45% (13/29). 3
The recurrence rate was 23.8% (5/21), and that the rate was lower (10%, 1/10) in patients treated with transcervical resection (TCR) and higher (36.4%, 4/11) among those treated with curettage or other therapies. 5
The pathology is characterized by biphasic proliferation of architecturally complex and cytologically atypical endometrial glands, typically with squamous metaplasia and a myofibromatous stromal component. 10 The pathogenesis is considered to be non neoplastic proliferation, possibly secondary to prolonged estrogenic stimulation of an endometrial stromal progenitor cell. Although whether there is any association between APAM and hormone therapy is unknown, APAM has been reported in patients receiving hormone therapy such as long-term tamoxifen therapy, estrogen supplementation therapy, 3 luteal hormone therapy, or clomiphene therapy.3,5 Thus estrogen-related factors have been considered to play an important role in the development of APAM.3,4 The curettage specimen obtained during the initial treatment in this case showed APAM with a markedly complex architecture of the glands, and the hysterectomy specimen showed endometrioid adenocarcinoma in continuity with APAM.
The MRI findings on T2 weighted image, APAM was seen as a slightly hyperintense polypoid mass mixed with markedly hyperintense foci that corresponded to islands of metaplastic endometrial foci histopathologically.11,12
Differential diagnostic considerations for a malignant uterine polypoid mass in the uterine cavity include endometrial stromal sarcoma, mixed mullerian malignant tumor, and endometrial carcinoma. Concomitant foci of endometrial carcinoma have been reported in about 7% of patients with APAM. 5 The PET-CT imaging showed an increased FDG uptake, the findings seems to be endometrial stromal sarcoma and atypical leiomyoma.
Therapy for APAM depends on multiple factors such as age at presentation and desire for childbearing among others. Because many patients are not only around 40 years but also nullipara, fertility-preserving treatment such as TCR have been performed as a conservative treatment and diagnosis.
Careful follow-up with ultrasonography, hysteroscopy, and endometrial biopsy should be performed, although appropriate intervals of examinations have not been clearly determined.
Conclusions
APAM may have a risk of recurrence or malignant transformation into endometrioid adenocarcinoma, and careful management is required if fertility is to be preserved. To our knowledge, this is the first report of PET-CT findings in APAM. Retrospective accumulations of case reports are mandatory.