
Abstract
Angiosarcomas are one of the rarest subtypes of sarcomas; those are malignant vascular tumors arising from vascular endothelial cells. Occurrence of intra-oral angiosarcoma is extremely rare (0.0077% of all cancers in Europe). We present here, to our knowledge, the first case of a 83-year-old man with gingival and both palatine tonsils localization of a grade-two angiosarcoma discovered after a two months history of a painful lesion followed by hematoma and spontaneous bleeding. Chemotherapy with paclitaxel and hemostatic radiotherapy were inefficient and he died seven months after the first symptoms. It is essential to use the vascular markers, such as CD34, CD31, ERG and FLI1, for a correct histological diagnosis, which remains difficult because it displays a wide range of morphological appearances and multiple patterns may be present in the same tumor. The main prognostic factors are chronic pre-existing lymphedema and tumor size greater than five centimeters. Malignancy grade and stage classification should be provided in all cases in which this is feasible because of predictive meaning. When possible, wide surgical resection with negative margins remains the cornerstone for the treatment of localized angiosarcomas, but despite the improvement of surgical techniques the prognosis is poor with more than half of patients died within the first year. Adjuvant radiotherapy is the standard treatment of high–grade (two and three), deep lesions, regardless of size, because it improved the local recurrence-free survival. For advanced disease, if possible, metastasectomy should be considered. The first-line chemotherapy with doxorubicin or paclitaxel should be discussed compared to best supportive care according to patient comorbidities and preference.
Introduction
A sarcoma is a malignant neoplasm that arises from transformed cells of mesenchymal origin. Sarcomas are rare tumors with an estimated incidence averaging 4-5/100,000/year in Europe. 1 There are 3000-4000 new cases per year in France. 2 Angiosarcomas are one of the rarest subtypes and represent 1-2% of all adult soft tissue sarcomas. 3 Those are malignant vascular tumors arising from vascular endothelial cells. In Europe, angiosarcomas incidence is approximately 0.31/100.00/year. Intra-oral soft tissue sarcomas prevalence is estimated at 0.14% of all head and neck cancers, or 0.0077% of all cancers. 4
This disease can affect patients of all ages and has a peak incidence in the seventh decade of life. It predominantly occurs in patients with chronic pre-existing lymphedema, which is an adverse prognostic factor for overall survival, local recurrence-free survival and distant recurrence-free survival. 3 Besides, tumor size greater than 5 cm is an adverse prognostic factor for overall and distant recurrence-free survivals. Performance Status (PS)>1 was also identified as the most significant risk factor for early death (<3 months) in advanced soft tissue sarcoma patients who were treated with first-line chemotherapy. 5
Case Report
We report here the case of a 83-year-old white man with a two months history of a painful lesion in the gingiva followed by hematoma in the right then left palatine tonsil with spontaneous bleeding (Figure 1). He complains of progressive odynophagia, dyspnea and weight loss. He has no antecedent beyond a benign prostatic hyperplasia. Complete blood cell count showed 12.3 g/dL hemoglobin and 400/mm3 lymphocytes. The coagulation factors are normal. A cervico-thoraco-abdominal computed tomography scan brings out tumoral syndrome in the two palatine tonsils with central necrosis (Figure 2). Furthermore two necrotic lymph nodes in right level Ib and right level IIa and one non-necrotic lymph node in left level IIa were present (Figures 3 and 4). The patient underwent bilateral tonsillectomy and nodal puncture in right level IIa. Histological diagnosis has been made according to the 2002 World Health Organization classification and a pathological expert second opinion has been asked in another reference center. The final pathological findings conclude angiosarcoma in the gingiva, both palatine tonsils and IIa right lymph node. Microscopic examination reveals the presence of a tonsil whose epithelial structures of the surface coating, as that of the crypts, are colonized by many polymorphic leukocytes, predominantly lymphocytes but also include some unaltered neutrophils. At the lymphoid apparatus exist prominent germinal center follicles. Sampling also includes at its periphery small lobules of seromucous glands and striated muscle bundles. Are also observed neoplastic structures that include vascular cavities bordered by a more or less dense and thick collagenous fibrosis, with a coating of atypical nuclei cells or tumor foci with rounded or globular cells whose cytoplasm is eosinophilic and whose nuclei contains clear chromatin with a prominent central nucleolus, often atypical (Figure 5). In some places the two (cavity and compact) aspects are in continuity. There are morphologically abnormal mitosis. There are six mitoses per ten fields at a magnification of 400. The tumor necrotic foci are rare. Immunohistochemical techniques were performed showing the following marks: marking of tumor cells for the CD31 antigen (clone JC/70A, Dako, 1/50) and CD34 (Clone QBEND, Cell Marque, 1/50). Marking of a part of the lesion for Actin (clone 1A4, Dako, 1/300) but not for BNH9 (clone Bnh9, Dako, 1/20). No marking for HHV8 (clone 13B10, Ventana, Prediluted). Furthermore the identification of KL1 (clone KL1, Immunotech, 1/200), epithelial membrane antigen (EMA) (clone E29, Dako, 1/200), CK5/6 (clone D5 16/B4, Dako, 1/50) pancytokeratin and P63 (clone 4A4, BIOSB, 1/100) shows no argument for carcinoma. Markings for the CD45 (clone 2B11 +PD7/26, Dako, 1/100), CD3 (polyclonal, DBS, 1/25) and CD20 (clone L26, THERMO SCIENTIFIC, 1/250) antigens do not argue for lymphoma. It is a grade two angiosarcoma (score 5 including 3 for differentiation, 1 for mitosis, 1 for necrosis). In the meantime the patient presents recurrent macroscopic hematuria, which require hemostatic surgery and several hospitalizations for transfusion. A month after the diagnosis a progression of the gingival tumor with bone involvement and a right tonsillar relapse were noted. Chemotherapy with paclitaxel 90 mg/m2 every week is initiated as first-line treatment. After five injections, deterioration of the general condition prevents further treatment. The patient underwent three sessions of hemostatic radiotherapy for oral bleeding, and likewise extreme exhaustion prevents further treatment. He died, seven months after the first symptoms and four months after the diagnosis of angiosarcoma, of gastrointestinal bleeding and mediastinal compression.

Necrosis painful tumor of right gingival and both palatine tonsils.
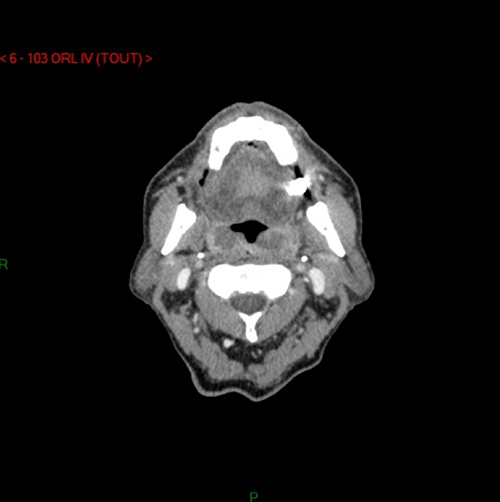
Cervical computed tomography-scan shows necrotic tumor of both palatine tonsils.
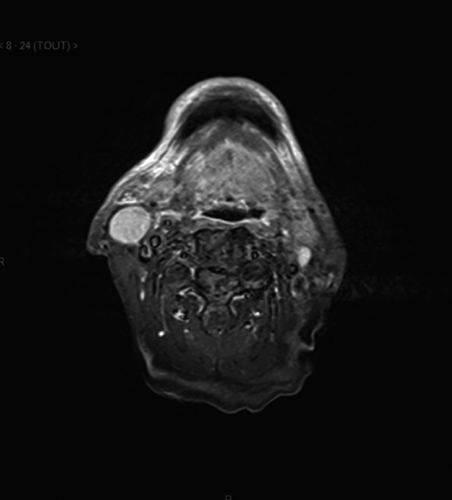
T2-weighted magnetic resonance imaging of lymph nodes in right level IIa and left level IIa, showing high density signals.

T2-weighted magnetic resonance imaging of necrotic tumor of gingiva and palatine tonsils.
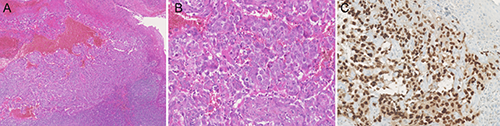
Oropahryngeal angiosarcoma with ulceration of the mucosae. Vascular proliferation on standard coloration with Hemalun Eosine Safron. A) magnification ×50; B) magnification ×200 and endothelial marker ERG expression; C) magnification ×200.
Discussion
Angiosarcomas are one of the rarest subtypes of sarcomas. Main primary sites are limbs (33 to 54%)3,6 and particularly the thigh, breast (20 to 35%),3,7 chest wall and trunk (30 to 35%)3,6 and head and neck (11 to 13%).3,6 Main metastatic sites are lung (25%), bone (22%), liver (16%) and brain (11%). 7 Intra-oral or salivary gland localization of angiosarcoma is pretty rare and few publications mention it (Table 1).8–28 Even if gingiva is, with tongue, the most common localization of this disease in literature, to our knowledge this report is the first case of gingival angiosarcoma with both palatine tonsils involvement.
Literature of intra-oral or salivary gland angiosarcomas.

Besides in the different articles, tonsil localization of angiosarcoma is always unilateral.
The malignancy grade should be provided in all cases in which this is feasible based on available systems, because it has prognostic and predictive meaning. The Federation Nationale des Centres de Lutte Contre le Cancer grading system is generally used, which distinguishes three malignancy grades based on differentiation, necrosis and mitotic rate. The American Joint Committee on Cancer/International Union against Cancer stage classification system stresses the importance of the malignancy grade in sarcoma.
The histopathologic diagnosis of angiosarcoma of soft tissue is difficult because it displays a wide range of morphological appearances ranging from areas of well-formed, anastomosing vessels to solid sheets of high-grade epithelioid or spindled cells without clear vaso-formation. Moreover, multiple patterns may be present in the same tumor. The vast majority of angiosarcomas of soft tissue are high-grade neoplasms with brisk mitotic activity, coagulative necrosis and significant nuclear atypia. Extensive hemorrhage is commonly present and may suggest a hematoma. Angiosarcomas express the typical vascular markers: CD34, CD31, ERG, FLI1 and occasionally podoplanin (D2-40).29–32 Some angiosarcomas co-express epithelial antigens, as keratins and EMA, allowing their distinction from carcinomas. 33 On genetics, high-level amplification of MYC in 8q24 is a consistent hallmark of radiation-induced and lymphoedema-associated angiosarcoma.34,35 VEGFR3 coamplification in 5q35 is detected in 25% of secondary angiosarcomas. Neither MYC nor VEGFR3 gene abnormalities have been reported in primary deep-seated soft tissue angiosarcoma nor radiation-associated atypical vascular lesions thus far.34,36
Wide surgical resection with negative margins remains the cornerstone for the treatment of localized angiosarcomas but despite the improvement of surgical techniques the prognosis is poor with more than half of patients died within the first year.6,7 Adjuvant radiotherapy is the standard treatment of high-grade (two and three), deep lesions, regardless of size, because it improved the local recurrence-free survival but did not influence overall nor distant recurrence-free survivals. For the others cases, radiation therapy should be discussed in a multidisciplinary setting. On the other side, (neo)-adjuvant chemotherapy did not influence overall, local recurrence-free or distant recurrence-free survivals. In a recent retrospective study, metastasectomy is associated with a major improvement of overall survival. 37 For metastatic disease the standard first-line treatment is chemotherapy based on anthracyclines. There is no formal demonstration that multi-agent chemotherapy is superior to single-agent chemotherapy with doxorubicin alone in terms of overall survival. In recent years, however, the insight has emerged that systemic therapy should become more tailored, in particular with respect to specific sarcoma histology. Besides weekly paclitaxel is an alternative option in angiosarcomas with similar efficacy demonstrated in several studies.37–43 The median overall survival is between 8 43 and 13.1 37 months, and the median progression-free survival is between 4 43 and 7.75 40 months with important differences in terms of doses and dosing schedules within studies. The response rate is between 45 43 and 89% 39 with neutropenia and peripheral neuropathy as most frequent toxicities. Considering the high risk of early death of patients who have poor PS, the decision to administer chemotherapy instead of best supportive care should be carefully assessed in this setting, given its potential lack of benefit. Because weekly paclitaxel and doxorubicin appears to have similar efficacy, the comorbidities, including cardiac ones, and the preference of the patients should be considered for the choice of the chemotherapy regimen.
Finally in phase II trials44,45 sorafenib, a small molecule B-RAF and VEGFR inhibitor, showed limited antitumor activity in pretreated with conventional chemotherapy patients only, for both visceral and superficial angiosarcomas, but tumor control was of short duration.
Conclusions
Angiosarcomas are aggressive tumors with poor prognosis. Chronic pre-existing lymphedema, tumor size greater than 5 cm, and PS>1 are the main adverse prognostic factors for overall survival. The histopathologic diagnosis is difficult and needs vascular markers expression. Grading and staging classification should be provided because of predictive meaning. When possible, radical surgery is required, followed by radiotherapy and/or chemotherapy. For advanced disease, if possible, metastasectomy should be considered. The first-line chemotherapy with doxorubicin or paclitaxel should be discussed compared to best supportive care according to patient comorbidities and preference.