
Abstract
Undifferentiated embryonal sarcoma of the liver (UESL) is a rare malignant hepatic tumor. A 47 year old male presented with symptoms of sour taste in his mouth, occasional nausea, indigestion and 15-pound weight loss over two months. He had an unremarkable upper gastrointestinal endoscopy. Imaging showed a large liver mass in the left hepatic lobe that was resected and then reported as UESL. He went on to develop lung metastases and was initially treated with doxorubicin and ifosfamide followed by switching of therapy to gemcitabine and docetaxel due to progression of disease. He had a good response after two cycles and went on to receive four more cycles, achieving stable disease. We can therefore conclude that the combination of gemcitabine and docetaxel is a potential therapeutic option for patients with UESL.
Introduction
Undifferentiated embryonal sarcoma of the liver (UESL) is a rare malignant hepatic tumor. Initially described as malignant mesenchymoma, mesenchymal sarcoma or fibromyxosarcoma, it was termed as UESL by Stocker et al. in 1978. 1 UESL refers to a heterogeneous group of tumors derived from mesenchymal tissues. It is usually seen in the pediatric population with peak incidence noted in children between 6 and 10 years of age. It is extremely rare in adults with less than 70 cases of UESL having been reported in patients above 15 years of age.2,3 While some studies have reported a slight female predominance in the adult population, others have not.4–6
Case Report
We present the case of a 47 year old male who presented with symptoms of sour taste in his mouth, occasional nausea, indigestion, as well as a 15-pound weight loss over two months. Initial physical examination and labs were unremarkable. He went to the local emergency room for evaluation after he had symptomatic tachycardia while exercising. He was admitted for further evaluation and had an upper gastrointestinal endoscopy which was unrevealing. This was followed by imaging of his liver which revealed a 15×13×11 cm liver mass in the left hepatic lobe.
Following this, he underwent a computed tomography (CT) scan of his chest, abdomen, and pelvis that also revealed the aforementioned liver lesion without any evidence of metastatic disease. Two weeks later, he underwent left lobectomy and resection of the liver mass.
The tumor showed pleomorphic spindled tumor cells arranged in fascicles with large zones of necrosis, a marked mitotic rate, interspersed foam cells, and focal areas that were more epitheloid and discohesive, with others that contained osteoclast-like giant cells. Immunohistochemistry revealed positive CD68 and caldesmon, with trace or weakly positive SMA, ALK-1, CD8/18 and AE1/AE3. All others were negative.
Final pathology was consistent with high grade spindle cell sarcoma with mild fibroblastic differentiation (Figure 1). As the liver represented the only site of disease, this was determined to represent a primary undifferentiated (embryonal) liver sarcoma. Tumor dimensions were 16×15.5×11.2 cm with a positive margin. Two of 2 celiac lymph nodes removed at the time of surgery were positive. Fluorescence in situ hybridization (FISH) was done for an Anaplastic Lymphoma kinase (ALK) gene rearrangement and was negative which ruled out inflammatory fibrosarcoma.
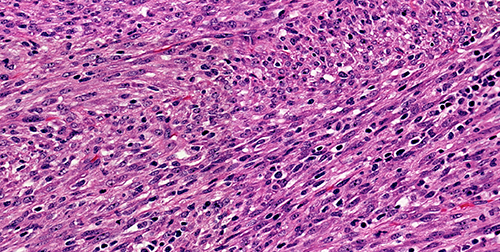
Hematoxylin and eosin stain at 400× magnification.
There was a delay in his care due the time it took for his pathologic diagnosis to be completed and as he moved back into this country and hence, two months later, CT showed significantly progressing disease and lung metastases. He was admitted to begin chemotherapy with dox-orubicin (25 mg/m2 IV for days 1 to 3) and ifosfamide (2.5 g/m2 for days 1 to 5). He received a total of two cycles after which he had significant progression of disease (Figure 2A) and was switched to gemcitabine (900 mg/m2 IV on days 1 and 8) and docetaxel (100 mg/m2 IV on day 8). He had a good response after two cycles (Figure 2B) and went on to receive four more cycles, achieving stable disease. His course was complicated by Pneumocystis jiroveci pneumonia after his primary physician placed him on steroids to aid his appetite without giving prophylactic antibiotics. After the 6th cycle of chemotherapy, he was admitted to a local hospital for worsening pneumonia. Due to a rapid decline in his performance status, he elected for hospice care. He died three weeks later.
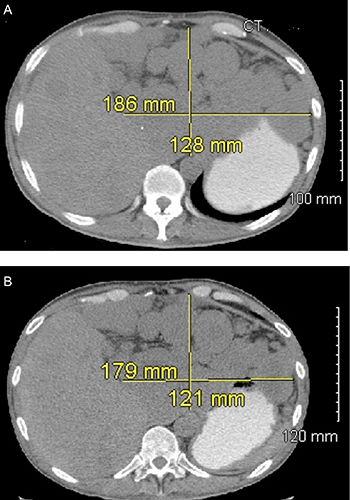
Computed tomography imaging before (A) and after (B) receiving gemcitabine and docetaxel.
Discussion and Conclusions
Although, the precise etiology of UESL is unclear, it is thought to be associated with multiple genetic mutations. Multiple cytogenetic studies have shown overexpression of p53 in more than 80% of these tumor cells, thus suggesting a role of p53 pathway in the pathogenesis of this tumor. 7 These studies have shown UESL to be associated with inac-tivation of the TP53 gene through the loss of heterozygosity and pathogenic mutation of the remaining allele leading to over expression. Studies have also shown UESL to have t(11;19)(q11;q13.3/13.4). Interestingly, UESL has known to share similar histological features and cytogenetic alterations as mesangial hamartoma of the liver, which is a benign tumor noted in pediatric population. This lead to the postulation that mesangial hamartoma could potentially progress to UESL with development of additional mutations. 8 Patients with UESL can present with a variety of nonspecific symptoms such as nausea, vomiting, abdominal pain, jaundice, weight loss and fatigue. 4 Painless abdominal distension secondary to the hepatic mass as well as spontaneous rupture of the tumor leading to intraperitoneal hemorrhage in rapidly growing tumors has been reported. 9 For unclear reasons, the right lobe is known to be more commonly involved than the left lobe, although simultaneous involvement of both the lobes have also been reported.4,5 Laboratory tests are of limited use as liver function can be normal or mildly deranged. 5 Serum alpha-feto protein usually remains normal but may be elevated in some cases.7,10
CT scan or magnetic resonance imaging (MRI) reveals a large space occupying lesion with mixed solid-cystic features. 11 These tumors are large with sizes ranging from 10 to 35 cm.5,12 The differential diagnosis for UESL include infectious etiologies such as an amebic liver abscess, intrahepatic hydatid cyst, polycystic liver disease, Caroli's disease, simple bile duct cyst, biliary cystadenoma, hamartoma, cystadenocarcinoma, bilioma. 13 PET scan and hydatid serologies can be done to narrow the differential diagnosis. Biopsy is often diagnostic. A pseudo-capsule with foci of extra capsular infiltration surrounds the tumor. UESL is composed of stellate and spindle shaped cells, set in myxoid matrix and areas of hyper cellularity. Moderate nuclear hyperchromasia and pleomorphism can also be seen. PAS positive, diastase resistant eosinophilic globules are typically seen within the cytoplasm. 14 Variable immuno-reactivity to desmin, vementin, cytokeratin, alpha1 antitrypsin, alpha 1 anti-chymotrypsin, CD34 antibodies has also been reported.2,12,15
UESL is a highly aggressive neoplasm with poor prognosis. While initial studies reported a median survival of less than 1 year after initial diagnosis more recent studies have reported the median survival to be closer to 2.5 years.1,2 The long term disease free survival was noted to be very poor even in patients who underwent complete surgical resection of the tumor. However, several recent reports have shown that the tumor can also be potentially curable.16–18 Surgical resection followed by chemotherapy remains the treatment of choice for patients with UESL, resulting in an improved overall survival.2,19 Neo-adjuvant or adjuvant systemic chemotherapy with combinations of doxorubicin, cisplatin or cyclophosphamide is often used and may improve survival.17,20 Combination chemotherapy regimens such as cisplatin with cyclophosphamide, doxorubicin or actinomycin D and/or vincristine have been used and have shown to be effective. 2 Radiotherapy has been used rarely. 21 In cases of recurrence, radical excision if feasible is recommended. 3 With the use of adjuvant chemotherapy, survival of greater than 10 years has also been reported. In patients with unresectable tumors and patients with spontaneous tumor rupture, prognosis is extremely poor. 12 Liver transplantations have been performed in the pediatric population with UESL with mixed results.22,23 This has however, not been reported in adults. Our case is unique since to the best of our knowledge, this is the first reported success of the combination of gemcitabine and docetaxel in UESL.