
Abstract
Ewing sarcoma is a primitive neuroectodermal tumor which seldom presents with primary disease in people over age 40 and outside of the appendicular or axial skeleton. We examine a case of primary thoracic Ewing Sarcoma diagnosed initially by CT-guided biopsy in a woman at the age of 74 years. The disease progressed after initial combined modality therapy consisting of neoadjuvant chemotherapy, surgical resection, and adjuvant radiation therapy and two additional courses of multiagent chemotherapy. After relapse of her disease, subsequent second- and third-line systemic agents which included chemotherapy and targeted agents were given with disease stabilization achieved now over 30 months from initial diagnosis. To our knowledge, this is the first report of a primary pulmonary Ewing sarcoma diagnosed in a patient greater than 70 years of age in whom multiple remissions have been achieved with tolerable toxicities.
Keywords
Method
The following is a report of a patient undergoing management of a pulmonary Ewing Sarcoma after treatment with vincristine, doxorubicin, cyclophosphamide alternating with ifosfamide and etoposide (VDC/IE) with progression; then transitioned to vincristine, topotecan, and cyclophosphamide alternating with ifosfamide and etoposide (VTC/IE), followed by surgical resection, and local radiotherapy. Upon disease progression, therapy was transitioned to irinotecan/temozolomide; and, after further progression, therapy was transitioned to regorafenib.
Introduction
Ewing Sarcoma denotes a family of aggressive primitive neuroectodermal tumors (PNETs) which, as a group, are the second-most common primary bone tumor of patients under 18 years of age. 1 Ewing Sarcoma is characterized by the ESWR1 rearrangement—a t(11;22) (q24;q12) translocation. 2 Most cases arise in the axial or appendicular skeleton. Only 30% are diagnosed in adults over the age of 30. 1 The disease is thought to be frequently sub-clinically metastatic at presentation as 80–90% of patients experience relapse after local therapy alone. 3 In metastatic disease, five-year survival rates of primary skeletal Ewing sarcoma have been observed to vary between 33% and 55%. 1 Poor prognosis is presaged by the presence of bone metastases with or without lung metastases at the time of diagnoses, primary axial disease, disease size greater than 100 mL at time of diagnosis, and relapse within 2 years of the original diagnosis. 1 Primary extraosseous presentation of Ewing sarcoma is rare and is mostly described in case reports and case series. In one retrospective review of all patients treated at a large children’s hospital system, only 46 cases of primary extraosseous disease were identified. 4 Patients with extraosseous disease were more likely to be female, of greater pediatric age, and have axial primary disease than those with osseous disease. 4 The mean age at time of diagnosis was 13. 4 Poor prognosis was found to be associated with stage at time of diagnosis; no association was observed with patient age, disease size, or disease location. Other large-scale case series included up to 57 patients.4–6 The oldest recorded case among these series was diagnosed at age 57 years4–6 In these case series, reduction in 5-year disease-free survival after management was observed to be associated with bulky disease >10 cm at time of diagnosis, metastatic disease at diagnosis, and suboptimal surgical margins. 5 Radiation therapy was significantly associated with reduced event-free survival but no association with overall survival was observed. 5
Primary Ewing sarcoma of the thorax is also exceedingly rare, and even more so in patients older than 40 years of age. One case report describes primary neuroectodermal tumor of the chest wall, also known as an Askin’s tumor, in a patient aged 63 with a protracted smoking history. 7 Three lesions were identified with regional destruction of the ribs. The diagnosis was established by pathologic analysis after CT-guided biopsy. That patient, however, died from an intrapulmonary infection before surgical, medical, or radiation therapies could be administered. We report our case of a 74-year-old female diagnosed with Ewing Sarcoma of the thorax whose disease remains in remission with acceptable toxicities on targeted therapy after two lines of dose-reduced neoadjuvant chemotherapy, surgical resection, adjuvant radiation, two lines of adjuvant systemic chemotherapy, and, after disease progression, salvage therapy with multi-target tyrosine kinase inhibition with regorafenib.
Case description
The patient is a 74-year-old female who presented with dyspnea and chest pain. She was found to have a transudative pleural effusion and initially underwent thoracentesis without evidence of malignant cytology. A left upper lobe pulmonary mass measuring 10 cm by 16.4 cm by 15.6 cm was detected on CT scan of the chest. Further, the left upper pulmonary lobe was collapsed without evidence of aeration with evidence of mass extension into the supraclavicular region and local compression of bronchi and vasculature. A PET-CT was subsequently performed. (Figure 1) A CT-guided biopsy was performed. Pathologic analysis showed an undifferentiated neuroectodermal sarcoma which stained positive for CD99 and FLI1. (Figure 2) The biopsy specimen was sent for molecular gene rearrangement studies and an EWSR1 rearrangement was detected. Axial (a) and coronal (b) fused PET-CT images show a large mass (arrows) in the left hemithorax with foci of increased metabolic activity. No metastatic disease is seen. Sections show small round cell tumor composed of undifferentiated round cells. Tumor cells are positive for CD99 and Fli-1 immunostains, focally positive for WT1 and negative for CK5/6, p63, TTF-1, chromogranin, synaptophysin, Melan-A, CD45, CD3, CD20, CD34, S-100, MPO and desmin. EWSR1 gene rearrangement detected at NeoDenomics Lab.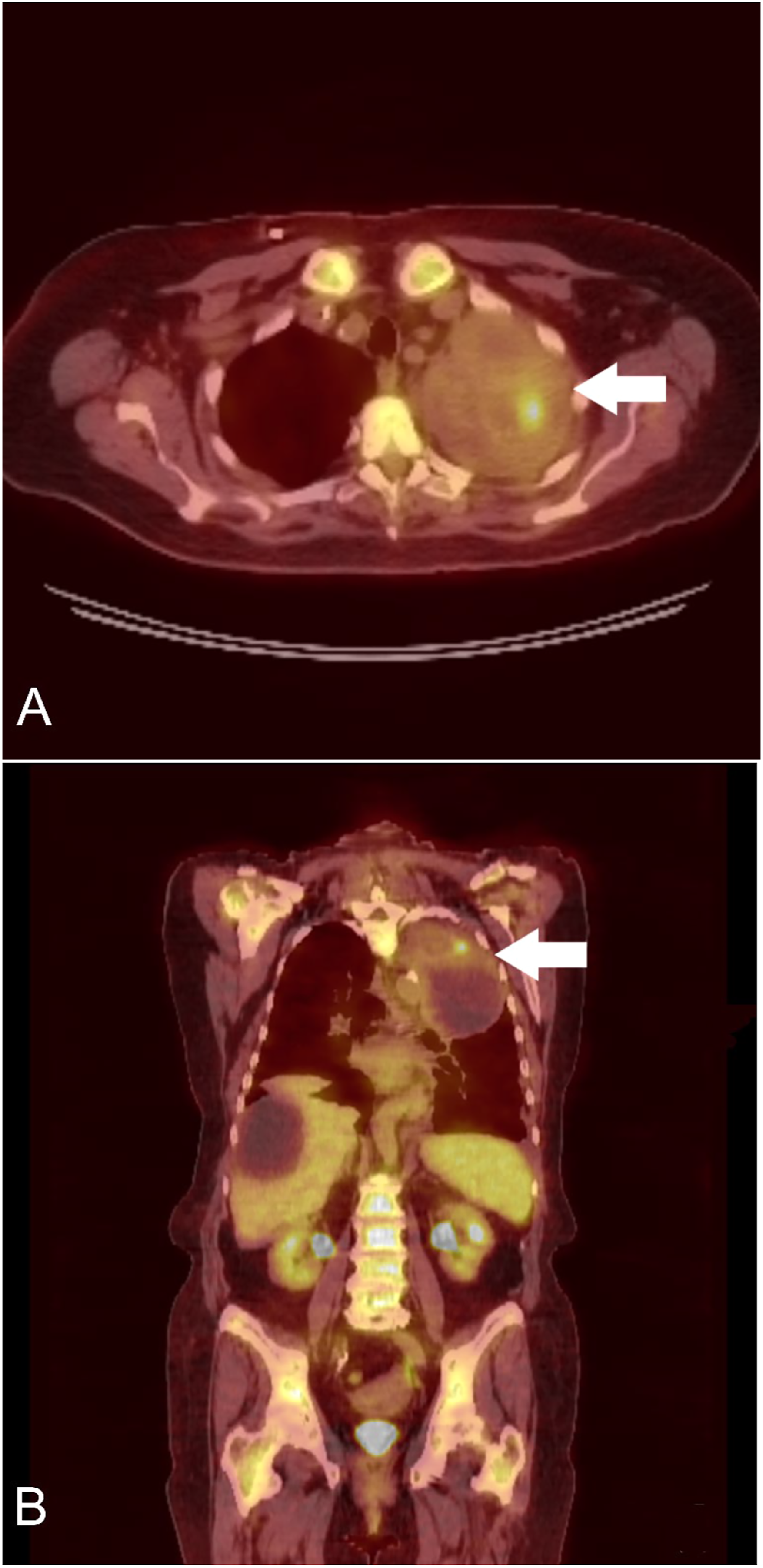

From February of 2018 to May of 2018, she was treated with four 21-day cycles of vincristine, doxorubicin, cyclophosphamide, and ifosfamide/etoposide (VDC/IE). The doses were attenuated due to her age. They consisted of doses of vincristine of 2 mg IV; doxorubicin of 60 mg/m2, and cyclophosphamide of 1000 mg/m2 with daily mesna at 60% of the cyclophosphamide dose. Ifosfamide and etoposide doses were given at 1800 mg/m2 on days 1–3 and 100 mg/m2 on days 1–3 every 21 days. No iron-chelation agents were given prior to doxorubicin infusion. During her VDC/IE therapy, she was treated with 4 total doses of 6 mg of pegfilgastrim, and her absolute neutrophil count (ANC) did not fall below 300,000 cells/mL during treatment. Her weight at the start of VDC/IE therapy was 77 kg and did not fall below 75 kg during treatment. Throughout her treatment course, she has been followed by a nutritionist. She tolerated oral nutrition well and did not require adjunctive therapy for dietary stimulation or mucositis.8,9 No evidence of malnutrition was noted.
After 4 cycles of VDC/IE, restaging scans showed no response to therapy. From May 2018 to August 2018, she was switched to 21-day cycles of vincristine 2 mg, topotecan 1 mg/m2, and cyclophosphamide 1000 mg/m2 per day with daily mesna at 60% of the cyclophosphamide dose were given for 3 days (VTC) alternating with the attenuated 3-day IE regimen. To tolerate the therapy, she was treated with 2 doses of 6 mg pegfilgastrim. Her ANC was not observed to fall below 300,000 cells/mL. Weight was stable during therapy and did not fall below 75 kg. Restaging scans in June 2018 showed response to therapy. Surgical resection was performed in August 2018; pathologic analysis of an intralesional specimen showed grossly positive margins and 50% necrosis. She underwent adjuvant radiation therapy until October 2018 receiving a total of 5,040 cGy over 28 fractions to the residual tumor. Her therapy was then followed by 2 cycles of adjuvant VTC. Unfortunately, a restaging PET/CT in March of 2019 of the thorax showed a nodular-appearing, pleural-based density in the left chest wall concerning for local recurrence with corresponding pain. She was transitioned to irinotecan 40 mg/m2 with temozolomide 100 mg/m2 over 5 days and completed 5 cycles from March 2019 to August 2019. A re-staging PET/CT showed significant improvement with some scarring in the area, but with increased metabolic activity in the acetabulum, a para-esophageal lymph node, an enlarged paraaortic nodule, and a hypermetabolic focus in the right proximal femur concerning new osseous metastasis. (Figure 3) In December 2019, she underwent palliative radiation to the right femur. Regorafenib was started after completion of radiation. Thus far, regorafenib has been well-tolerated with only one delay in therapy due to thrombocytopenia and hyperbilirubinemia. Weight has been stable at a range of 77 kg–81 kg and nutritionist assessments are without concern for malnutrition. Oral mucositis or other dose-limiting toxicities were not observed. No neutropenia was observed and no treatment with granulocyte colony-stimulating factors was administered during regorafenib therapy. As of June 2020, she had completed seven cycles of regorafenib in total. Restaging PET-CT scans have shown improvement with no recurrence or new metastatic disease (Figure 4). Coronal maximum intensity projection (MIP) image of PET-CT, shows new metabolic activity (long white arrow) in right paraesophageal lymph node, a metastatic focus in the right proximal femur (arrowhead), and another metastatic focus in the left acetabulum (squiggly arrow). Note increased metabolic activity in a paraaortic nodule lymph node (black arrow) in the epigastrium, felt to be reactive enlarged lymph node. Coronal maximum intensity projection image from the most recent PET-CT shows near complete resolution of metabolic hyperactivity in the paraesophageal lymph node. Post radiation changes are seen in the right upper thigh. The activity in the left acetabulum has decreased with central area of absent activity suggesting central necrosis. The activity in the presumed reactive lymph node in the epigastric region has also returned to normal.

Discussion
In case reports, Ewing sarcoma of the chest wall, also known as Askin’s Tumor, has been noted to present as acute bacterial pneumonia or acute dyspnea. In this case, a CT of the thorax at presentation showed a 10 cm × 16 cm × 15 cm left upper lobe mass spreading into the supraclavicular region, resulting in total collapse of the left upper lobe, compression of local bronchi and vasculature, and a small pleural effusion
In the reported case, surgical resection resulted in positive margins, and the patient underwent local radiation of the left upper pulmonary lobe. Radiation therapy has been studied most extensively in appendicular skeletal disease and is most commonly used in patients who are poor surgical candidates or as adjuvant therapy after surgical resection with positive margins. 13
The reported patient received irinotecan, temozolomide, and vincristine as a second-line therapy, a strategy which carries a 2A recommendation from the NCCN. 10 Unfortunately, among second-line chemotherapies for Ewing sarcoma in adults, there are no comparative studies to suggest a superior approach. 14 A major multicenter study of treatment of refractory PNET with combined irinotecan and temozolomide included 34 patients older than 18 years of age and demonstrated increased overall survival and improved Eastern Cooperative Oncology group (ECOG) performance status after 1 year of therapy. 12 The study noted that ECOG performance status and lactate dehydrogenase (LDH) levels were predictive of response. 12 In the reported case, ECOG was consistent at 1–2, portending a positive outcome. An LDH was not followed. NCCN guidelines also include Cabozantinib as a category 2A recommendation for second-line therapy for treatment of advanced Ewing’s sarcoma. Cabozantinib is a small molecule inhibitor of VEGFR2 and c-Met which is FDA-approved to treat medullary thyroid cancer. In a single-arm phase II study of 39 ECOG 0-1 patients with documented Ewing sarcoma disease progression after first-line therapy who were treated with cabozantinib, a partial response was observed in 26% of treated patients and 6 months of progression-free survival was observed in 33% of treated patients. 15 Other second-line therapies for Ewing’s sarcoma with category 2A recommendations by the NCCN include cyclophosphamide and topotecan with or without vincristine; and docetaxel and gemcitabine. 10
After progression on irinotecan/temozolomide, the reported patient was treated with regorafenib, a multi-kinase inhibitor which is thought to have activity against vascular endothelial growth factor 1 (VEGF1); VEGF2; VEGF3; platelet-derived growth factor beta (PDGF 1a); fibroblast growth factor FGFR1; and the mutant oncogenic kinases c-KIT, RET, B-RAF, and TIE2. 16 Although regorafenib was originally approved by the FDA for gastrointestinal and hepatocellular cancers, its potential in managing bone cancer was validated in a 45-patient placebo-controlled randomized control trial including patients with metastatic osteosarcoma progression on one or two lines of chemotherapy and high functional status. 17 In that study, 66% of patients randomized to regorafenib were observed to be progression-free at 8 weeks. In comparison, all patients in the placebo arm experienced progression at 8 weeks 17 Grade 3 adverse events observed in the regorafenib group included hypertension and hand-foot skin disease, neither of which were observed in the presented case. Regorafenib salvage therapy for Ewing Sarcoma is an area of active investigation. A randomized, double-blinded phase II study of regorafenib in the treatment of advanced soft tissue sarcoma, the REGOSARC trial, suggested an improvement in progression-free survival for all non-adipocytic soft tissue sarcomas. 18 Further, the strongest association between treatment and progression-free survival was observed in the “other sarcoma” cohort, which included diseases histologically and clinically most similar to Ewing sarcoma. 18 This trial was followed by the SARC024 trial, which included a single-arm, phase II subgroup trial of regorafenib in Ewing sarcoma of the soft tissue and bone in 30 adult (>18 year old) patients which had progressed on at least one line of conventional chemotherapy. 19 In that trial, a median progression-free survival of 3.6 months (95% CI 2.8–3.8 months) was observed. In the reported case, one scheduled dose of regorafenib was held due to thrombocytopenia and hyperbilirubinemia, but the treatment has otherwise been well-tolerated without significant dose-limiting adverse effects after dose adjustment. In the SARC024 study, the most frequent dose-limiting toxicities observed were hypophosphatemia, hypertension, and high ALT; thrombocytopenia nor hyperbilirubinemia were not observed. NCCN treatment guidelines for refractory Ewing sarcoma do not presently include regorafenib. 10
Other multi-target tyrosine kinase inhibitor salvage therapies for refractory PNETs are currently under investigation. Pazopanib, a multi-target tyrosine kinase inhibitor, is approved for the treatment of soft tissue sarcoma refractory to first line doxorubicin-based chemotherapy regimens. In the phase III Pazopanib for Metastatic Soft-Tissue Sarcoma (PALETTE) study, amongst patients with heterogenous soft tissue sarcomas who had experienced progression on one line of chemotherapy, pazopanib therapy showed a promising progression free-survival benefit compared with a placebo-controlled arm. 20 In that study, two Ewing sarcoma cases were included. However, both cases were included in the placebo control arm. One case report demonstrates sustained regression of a thoracic Ewing sarcoma refractory to first-line VDC/IE in a 48-year old man on pazopanib. 21 Other case reports detailing patients with refractory Ewing sarcoma with different primary tumor sites in whom regression was achieved with pazopanib have been published.22,23
Conclusion
The reported patient serves as a highly unusual example of Ewing sarcoma of the chest wall presenting in a previously healthy 74-year-old woman who has, remarkably, been maintained on regorafenib after progressing on several lines of therapy. She was managed with neoadjuvant VDC/IE and VTC chemotherapies, surgical resection with positive margins, localized radiation therapy, and adjuvant VDC/IE and VTC chemotherapies. After pulmonary recurrence was observed on PET/CT, she was treated with five cycles of irinotecan/temozolomide therapy. After a second recurrence was observed, she was treated with regorafenib and has experienced continued remission with acceptable toxicities. Screening for recurrence is ongoing. This unusual case suggests the applicability of established NIH and NCCN treatment guidelines for Ewing Sarcoma, most thoroughly studied in pediatric, osseous forms of Ewing Sarcoma, to geriatric patients with new primary disease and to patients with primary Ewing sarcoma of the chest wall and lungs. It prompts further investigation into whether reduced-dose first-line VDC/IE and VTC chemotherapies are appropriate in Ewing sarcoma patients of advanced age. It also prompts further study of regorafenib and other multi-target target kinase inhibitors as a treatment strategy for recurrent Ewing Sarcoma in adult patients.
Footnotes
Acknowledgements
We would like to thank the patient for her participation in this study.
Contributorship
RMT wrote the draft of the manuscript. KL and JH reviewed and edited the manuscript. DP provided formatted radiology images and interpretation. AF provided pathology slide images and interpretation. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Keck Medicine of USC
Informed consent
Written, informed consent was obtained from the patient for their anonymised information to be published in this article.