
Abstract
We report a case of KL-6 producing peritoneal malignant mesothelioma. A 56-year-old woman was referred to our hospital on November 2005 with severe abdominal distention. Peritoneal malignant mesothelioma with epithelioid type was diagnosed by clinical symptoms, laboratory investigations, imaging studies, and immunohistochemical examination of known tumor markers. In addition, high serum and ascitic KL-6 levels were observed and the immunostaining of the tumor for KL-6 was evident. We thus consider KL-6 to be a potential novel marker for peritoneal malignant mesothelioma with epithelioid type.
Introduction
Malignant mesothelioma is an aggressive neoplasm of serosal surfaces, i.e., pleura (65-70%), peritoneum (30%), tunica vaginalis testes, and pericardium (1-2%). 1 Peritoneal malignant mesothelioma is clearly confined to the peritoneal cavity lined by visceral and parietal peritoneum. The risk of peritoneal mesothelioma increases with age and always difficult to diagnose due to common and non-specific clinical presentation as well as due to lack of definite laboratory investigation and histochemical marker. Immunohistochemically, there is no specific marker for early diagnosis of peritoneal malignant mesothelioma. Recent studies have focused on Krebs von den Lungen-6 (KL-6) as a candidate for tumor marker. KL-6 is a human MUC1 mucin protein that is moderately expressed in type II pneumocytes, respiratory bronchial epithelial cells, and gastric fundic gland cells. 2 KL-6 is strongly produced by regenerating type II pneumocytes in interstitial lung diseases, and thus it has been documented as a highly specific and sensitive marker of the disease activity.3,4 In this study, we report a case of peritoneal malignant mesothelioma in a woman without known exposure to asbestos and assess the diagnostic utility of KL-6.
Case Report
A 56-year-old woman with a height of 157 cm and weight of 55.1 kg presented to the outpatient clinic having the history of abdominal distention since September 2005 and was referred to our hospital on November 2005. She worked at an iron factory for 4 years without known exposure to asbestos. She had no history of pain, abdominal mass, significant weight loss, dyspnea, cough, chest pain, or constitutional symptoms. In addition, she had no other relevant past medical and surgical history or no significant drug history. Her travel, family and social histories were unremarkable.
On presentation, she was non-anemic, non-icteric, her blood pressure was 139/84 mmHg, heart rate 87 beats/min and temperature 36.8°C. Peripheral lymph nodes were not palpable. The physical examination revealed that her abdomen was soft and non-tender but much distended. No masses were palpable, but massive ascites was pointed out. Laboratory analysis revealed thrombocytosis, hypoalbuminaemia and elevated C-reactive protein. The white blood cell count, erythrocyte count, renal function tests and level of serum electrolytes were normal. Liver function test yielded elevated level of ALP (292 IU/L) and LDH (159 IU/L). However, AST, ALT, γ-GTP, AMY levels were normal. Serum total cholesterol and triglycerides were also normal. The level of carcinoembryonic antigen (CEA), alpha-fetoprotein (AFP), carbohydrate antigen19-9 (CA19-9), carbohydrate antigen125 (CA125), and CYFRA in serum were found to be within normal limit. Serum KL-6 was examined for early detection of interstitial pneumonia which might be a potential adverse effect of chemotherapy. It was unexpectedly elevated at 9000 IU/mL (normal up to 500 IU/mL). CT scans revealed thickened greater omentum with massive ascites (Figure 1A) but no lung tumor or interstitial pneumonia. FDG-PET scan demonstrated positivity in the peritoneum (Figure 1B) and negativity in the ovary. Diagnostic paracentasis yielded yellow exudative fluid (Protein 5.2 g/dL), 1.036 specific gravity (normal up to 1.016) and showed 3610 total cells with predominance of mononuclear cells. CA125 and KL-6in ascites fluid was 86 U/L and 7500 U/mL, respectively. The level of hyaluronic acid in serum and peritoneal fluid was at 60 ng/mL and 11,900 ng/mL, respectively. Cytological examination suggested the possibility of peritoneal mesothelioma, but it was insufficient for the diagnosis. Diagnostic laparoscopy along with peritoneal biopsy was performed to obtain histopathological and immunohistochemical analysis for establishing the definitive diagnosis. Laparoscopy showed multiple yellowish small nodular lesions of the peritoneal surface and the thickened greater omentum. Hematoxylin and Eosin (H&E) stain at low magnification revealed sheet like epithelioid tumor cells with monotonous and bland in appearance (Figure 2A) and higher magnification showed oval shaped mesothelioma cells, with indistinct border, moderate cytoplasm, and prominent nuclei with inconspicuous nucleoli (Figure 2B). Microscopic features were consistent with peritoneal mesothelioma with epithelioid type. In addition, immunohistochemical stains were performed with the avidin-biotin peroxidase complex (ABC) method (LSAB kit; Dako, Carpinteria, CA) using antibodies against AE1/AE3, cytokeratin 5/6 (CK5/6), epithelial membrane antigen (EMA), calretinine, WT-1, D2-40, CEA, MOC-31, Ber-EP4, and thyroid transcription factor (TTF)-1. Staining procedures were conducted according to the manufactures’ instructions. The neoplastic cells showed strong positivity for AE1/AE3 (Figure 3A), moderate surface positivity for calretinine (Figure 3B), and surface and cytoplasmic positivity for CK 5/6, strong surface positivity for EMA, nucleonic positivity for WT-1, and weak surface positivity for D2-40 (data not shown). The tumor cells are completely negative for CEA, MOC-31, Ber-EP4, and TTF-1 (data not shown). All of these pathological results were compatible with peritoneal malignant mesothelioma with epithelioid type. Based on the serum elevation of KL-6, we examined KL-6 by immunohistochemistry using the anti KL-6 antibody (kindly provided by Eisai Co.) as described elsewhere, 5 revealing distinct surface positivity for the mesothelioma cells (Figure 3C). Fuzzy and fluffy pattern was evident for ascitic tumor cells (Figure 3D). Sequential four regimens of palliative chemotherapy including gemcitabine plus cisplatin, paclitaxel plus carboplatin, irinotecan plus cisplatin, and pemetrexed plus cisplatin were administered and serum KL-6 level was monitored. After the chemotherapy with gemcitabine plus cisplatin, serum and ascitic KL-6 once dropped, but these levels increased in association with worsening of the disease. Despite chemotherapy, the patient died 32 months after the initial diagnosis.
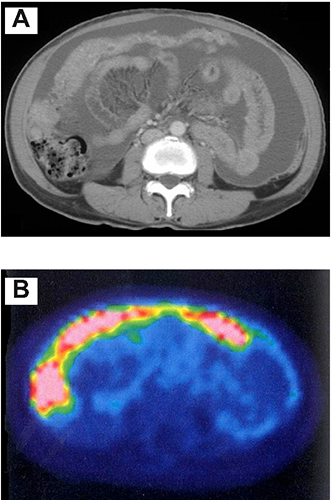
Imaging studies. A) Computed tomography scan of the abdomen showing massive ascites and thickened greater omentum. B) FDG-positron emission computed tomography scan showing strong positivity in the peritoneum.

Pathological findings of the peritoneal malignant mesothelioma. A) The tumor is composed of sheet like epitheloid cells with monotonous and bland in appearance (Hematoxylin and Eosin, 50×). B) Higher magnification of the tumor cells showing oval shaped mesothelioma cells, with indistinct border, moderate cytoplasm, and prominent nuclei with inconspicuous nucleoli (Hematoxylin and Eosin, 200×).

Immunopathological findings of the peritoneal malignant mesothelioma. A) The tumor cells showed strong positivity for AE1/AE3, B) moderate surface positivity for calretinine, and C) strong surface positivity with KL-6. D) The ascitic tumor cells showed fuzzy and fluffy surface with KL-6. Magnification 200×.
Discussion
Asbestos is the major carcinogen associated with malignant mesothelioma. 6 However, half of the patients with malignant mesothelioma of the peritoneum have not exposed to asbestos, 7 as in this case. Despite recent progress of multidisciplinary therapy including surgery, chemotherapy, radiotherapy, and gene therapy, the median survival is 10 months and relative 5-year survival is 16%. 7
The important differential diagnosis of malignant mesothelioma of the peritoneum includes serous carcinoma of the peritoneum and metastatic serous carcinomas of the ovary. 8 Immunohistochemical panels are important to establish the differential diagnosis. Malignant mesothelioma is characterized by the presence of positive staining for calretinine, EMA, CK5/6, WT1, D2-40, mesothelin and the absence of staining for CEA, CA19-9, Ber-EP4, MOC-31, or TTF-1.6,8 To the best of our knowledge, this is the first case report of KL-6 producing peritoneal malignant mesothelioma. KL-6 has been the established serum and immunohistochemical marker for diagnosing interstitial lung diseases and is widely applied to clinical practice.2–4 In addition, immunohistochemical assessment of KL-6 has been increasingly applied to diagnose various types of neoplasms, including gastrointestinal, hepatic, pancreatic, and ovarian cancers. 9 Especially, it has been an excellent immunohistochemical biomarker in association with a micropapillary pattern in breast, urinary bladder, and gastric carcinomas and it stains linearly along the surface of the cancer cells without staining of the cytoplasm, manifesting inside out pattern.10,11 In our case, there was distinct surface positivity with fuzzy and fluffy pattern for KL-6 of the mesothelioma cells. Several ultrastructural studies have shown that the mesothelioma cells exhibited long thin, occasionally branching surface microvilli.12–14 This finding has been considered as the most remarkable and reliable morphological feature of malignant mesothelioma cells. 13 Although we did not perform electron microscopic studies of mesothelioma cells, there may be a possibility that fuzzy and fluffy surface staining for KL-6 may indicate the surface microvilli. A recent study has identified serum soluble mesothelin-related protein (SMR) could be a useful marker for malignant mesothelioma. 15 Fukuoka et al. improved its diagnostic performance by combing serum SMR and CEA. 16 Our present study has shown that serum KL-6 can be regarded as a potential tumor marker in peritoneal malignant mesothelioma with epithelioid type. Serum KL-6 levels should be evaluated in screening for malignant mesothelioma among those who had been exposed to asbestos in future studies. As for KL-6 as a serum tumor marker, it has been useful in diagnosing several types of cancers. Kohno et al. have first reported its usefulness in diagnosing lung adenocarcinoma, pancreatic cancer, and breast cancer. 17 They also emphasized that its elevation correlated with tumor progression. A recent large scale case-control study has further confirmed that serum KL-6 is associated with subsequent lung cancer among patients with interstitial lung disease. 18 Recent studies have strengthened its diagnostic value in breast cancer and hepatocellular carcinoma.19,20 Although further work is needed, our findings support a potential role of serum, ascitic, and immunohistochemical evaluation with KL-6 for tumor etiology and early diagnosis in peritoneal malignant mesothelioma. Therefore, the utility of KL-6 for monitoring tumor progression should be established by studying more accumulated cases in future.
Conclusions
In summary, we are the first to describe the serum examination and immunohistochemical study of KL-6 for peritoneal malignant mesothelioma. Future studies are needed to further characterize the molecular features of KL-6 associated with this tumor and to determine its clinical value.
Footnotes
Acknowledgements
The authors are grateful for the technical assistance of Mr. Y. Okada (Matsuyama-shimin Hospital, Matsuyama, Japan).