
Abstract
Perineal leiomyosarcoma is an extremely rare and aggressive cancer with a high metastatic potential and no defined standard treatment. There are only a few (six) reported cases in the literature. We report the case of a 67-year-old woman with a perineal leiomyosarcoma arising at the same site of a previously resected superficial angiomyxoma. Initially, she was treated for a presumptive recurrence of angiomyxoma. As she did not respond to medical therapy, she underwent repeat surgical excision. Pathology revealed a high grade leiomyosarcoma, histologically strikingly distinct from the initial diagnosis. She received adjuvant local radiation therapy, and remains without evidence of recurrent disease 36 months after completion of all therapy. This is the first reported case of a high grade perineal leiomyosarcoma originating at the same site as a resected benign superficial angiomyxoma. Our case emphasizes the necessity of a prompt histological diagnosis in cases of presumed recurrent perineal angiomyxoma.
Case Report
A 67-year-old Caucasian female presented to our clinic for the management of a recurrent perineal mass. Fourteen months prior, she had similar complaints and was diagnosed with superficial angiomyxoma of the perineum after surgical resection of the mass from the left paravaginal and pararectal space. The margins were negative. Immunohistochemistry of this 5×3×2.5 cm benign myxoid lesion was positive for smooth muscle actin and estrogen receptor, and negative for desmin and caldesmon. A diagnosis of superficial angiomyxoma was made (Figure 1). Two months after the procedure, she noted swelling with pain at the surgical site. A magnetic resonance imaging (MRI) of the pelvis confirmed a recurrent mass (6.4×6.2×8.5 cm) at the same site and was presumed to be a recurrent angiomyxoma. Biopsy was not obtained. The patient was started on anti-estrogen therapy with tamoxifen. She was continued on tamoxifen for a total of 8 months with very minimal resolution of her clinical symptoms. A repeated MRI revealed increasing size of the mass, for which she was switched to an aromatase inhibitor, letrozole. The patient was referred to our facility after 6 weeks of letrozole did not seem to provide any clinical or radiological benefit. The patient had a history of uterine leiomyoma for which she underwent a total abdominal hysterectomy and bilateral salpin-go-oophorectomy twenty-two years prior to this present presentation. She also had a history of vaginal dysplasia and was treated with excision sixteen years prior to presentation. At our first clinical visit, the patient complained of persistent pain in her perineal region, with noticeable discomfort in a seated position. She denied complaints with bladder or bowel habits. She denied any weight loss, fever or vaginal bleeding. A recto-vaginal examination revealed a large mass within the perineum, extending into the buttocks. MRI demonstrated a hypervascular, well circumscribed 9.8×8.1×8.8 cm ischioanal fossa tumor with considerable mass effect on adjacent structures but without invasion (Figure 2). Pelvic lymph nodes were not involved radiologically and the metastatic workup was negative.
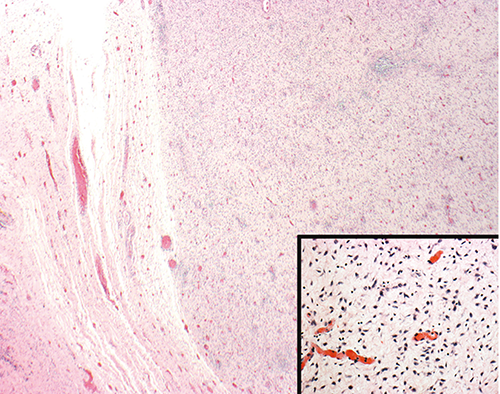
Multilobulated hypocellular tumor (angiomyxoma) with circumscribed borders composed of bland stellate and spindled cells in a loose stroma with scattered thin walled vessels and sparse inflammation (Hematoxylin & Eosin, ×2). Inset: Hematoxylin & Eosin, ×20.
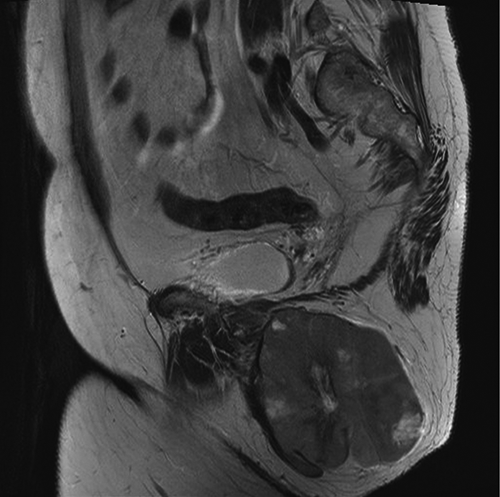
Magnetic resonance imaging scan demonstrating a hypervascular, well circumscribed 9.8×8.1×8.8 cm ischioanal fossa tumor with considerable mass effect on adjacent structures but without invasion.
The presumptive radiological diagnosis was recurrent angiomyxoma. She underwent embolization of the feeding vessels prior to the surgical resection, which involved a complete excision of the mass without entry into the capsule of the tumor. There was no local invasion of any surrounding structures. This was followed by a gracilis muscle flap closure of the resultant perineal defect. The resected tumor measured 11.5×10.0×9.5 cm and weighed 402 grams. Histopathology revealed a high grade spindle cell neoplasm characterized by marked cellularity and pleomorphism with increased mitotic activity (>5 per 10 high power fields) and areas of necrosis (Figure 3). Immunohistochemistry showed positive immunoreactivity of the tumor cells for actin and desmin while S-100, CD117 and keratin AE1/AE3 were negative, confirming the diagnosis of a high grade leiomyosarcoma. The anal margin was involved by tumor. The previously excised specimen from 14 months ago was compared to the current tumor with the former demonstrating a multilobulated hypocellular tumor with circumscribed borders composed of bland stellate and spindled cells in a loose stroma with scattered thin walled vessels and sparse inflammation consistent with a diagnosis of superficial angiomyxoma (Figure 1). No atypia, increased mitotic activity or necrosis was present. She underwent adjuvant radiation therapy receiving 60 Gray in 30 fractions to the post-operative bed involving the left perineum and pelvis followed by a boost of 6 Gray in 3 fractions to the area of positive margin along the anal canal (total dose: 66 Gray in 33 fractions.) She was also offered adjuvant chemotherapy with adriamycin and ifosfamide, which she declined. She has had close follow-up clinical exams and imaging for the last 36 months, without any recurrence of her disease.

High grade spindle cell neoplasm (leiomyosarcoma) with marked cellularity and pleomorphism with increased mitotic activity and areas of necrosis present elsewhere in the tumor (Hematoxylin & Eosin, ×20).
Discussion
Soft tissue sarcomas are rare cancers with an annual incidence of less than 5 per 1,000,000. 1 This comprises 0.7-1% of all cancers diagnosed annually, with leiomyosarcoma being one of the most common. As per the SEER data, higher incidences of leiomyosarcomas were noted in white females. Advanced grade, stage and age at diagnosis were independent markers of poor survival. The uterus and retroperitoneum were reported to be the most common anatomical sites involved. 1
Perineal leiomyosarcoma represents a very rare entity and an extensive search of the English literature reveals only a few documented case reports.2–6 These are aggressive tumors with no defined standard treatment protocol. Complete surgical excision is considered the treatment of choice, irrespective of the histological grade. The close proximity of these tumors to multiple vital organs often prevents complete resection with negative surgical margins. Adjuvant radiotherapy becomes imperative especially in cases with positive margins. The role of adjuvant chemotherapy is not well well-defined. Prospective clinical trials examining the use of adjuvant chemotherapy and/or radiation therapy are needed to validate their use in treatment of these rare tumors of the perineum.
The role of Positron emission tomography-computed tomography (PET-CT) scans in post-therapy surveillance to detect recurrence in asymptomatic patients with history of uterine leiomyosarcoma showed promising results. 7 MRI seems to be the best diagnostic tool to characterize these lesions. Radiologically, leiomyosarcomas commonly present as soft tissue masses with low intermediate signal intensity on T 1 weighted images and high signal intensity on T2 weighted images. 8
Histologically, they are composed of highly cellular fascicles of spindle shaped cells and elongated nuclei with blunted
Conclusions
To the best of our knowledge, this is the first reported case of a high grade perineal leiomyosarcoma originating at the same site of a resected benign superficial angiomyxoma. Our case also emphasizes the necessity of a prompt histological diagnosis in cases of presumed recurrent perineal angiomyxomas. It also challenges the role of any adjuvant chemotherapy in cases of leiomyosarcoma.