
Abstract
A 49-year-old female presented with an aggressive pelvic angiomyxoma (AAM). The completely resected specimen revealed the usual myxedematous tumor with a nodule inside it. Histopathologically, the myxedematous area consisted of bland spindle-shaped cells in the background of blood vessels of varying calibers, and the nodule was composed of tumor cells with epithelioid features. In the nodule, cellularity was increased and nuclear enlargement was observed, but nuclear atypia was not significant and mitotic figures were scarce. Immunohistochemically, both components were positive for desim, αSMA, estrogen receptors, and progesterone receptors. However, they were negative for AE1/3, EMA, S100, CD34, HMB45, and Melan A. The MIB-1 labeling index was 5.8% in the nodule and 1ess than 1% outside it. The nodule was therefore considered a benign component of AAM. To the best of our knowledge, the presence of such a nodule in AAM has not been reported previously.
Introduction
Aggressive angiomyxomas (AAMs) are rare mesenchymal neoplasm arising especially in the soft tissue of the pelvic and perineal region. Its peak incidence is known to be in young women in the third and fourth decades of life. 1 In a study of more than 100 cases, the female to male ratio was 6.6:1. 2 Steeper and Rosai first reported the tumor in 1983, 3 with a case series of 9 female patients, each of them having a propensity for local recurrence. The tumor was therefore called aggressive. Resected margins are often positive because AAMs are poorly delineated and infiltrate adjacent soft tissue. Tumor recurrence is a primary cause of patient morbidity, and recurrence rates range from 25% to 47%, as described in large case series.2,4,5 Histopathological examination usually reveals a paucicellular tumor composed of bland spindle-shaped cells in a myxedematous background with blood vessels of varying calibers. 3
We here report a rare case of AAM in the pelvic cavity containing a cellular nodule. Most areas of the tumor showed the usual histopathological features, but a distinct cellular nodule inside it displayed an epithelioid change in the tumor cells. It has not recurred for 1 year after the total surgical resection negative for surgical margin. To the best of our knowledge, the presence of a nodule with epthelioid tumor cells in AAMs has not been documented in the literature.
Case Report
A 49-year-old female was admitted to a nearby hospital with a chief complaint of genital bleeding. Abdominal ultrasonography revealed an intrapelvic mass, and she was referred to our hospital. Computed tomography and magnetic resonance imaging revealed a huge mass in the pelvic cavity. T2-weighted images (Figure 1A) and diffusion-weighted images (Figure 1B) showed high intensity consistent with a tumor. Under the diagnosis of an ovarian tumor, the operation was performed, and the mass was found to arise from the retroperitoneum. Total resection was completed, and the surgical margin was found to be histopathologically negative. After the operation, the patient was regularly monitored. No apparent recurrence was detected on magnetic resonance imaging 1 year after operation.

Magnetic resonance imaging of the tumor. A) A T2-weighted image showing a high intensity mass in the pelvic cavity. A nodule with moderate intensity present inside it (arrow). B) A diffusion-weighted image displaying a nodule with high intensity inside the mass.
Macroscopic examination revealed a myxedematous tumor (size, 18×13×5 cm; Figure 2A). The cut surface showed a yellowish-white and elastic hard nodule (size, 1.5×1.5 cm) (Figure 2B).
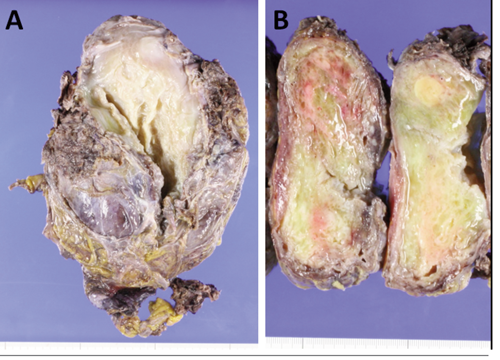
Macroscopic findings of the tumor. A) A surgically resected specimen showing a mass (size 18×13×5 cm). B) A myxedematous cut surface of the tumor. A solid and yellowish-white nodule (size, 1.5×1.5 cm) present inside it.
Microscopically, the tumor was composed of spindle-shaped cells sparsely scattered in the myxedematous background along with vessels of varying calibers (Figure 3A). Higher magnification demonstrated that the spindle-shaped cells had bland nuclei (Figure 3B). Mitotic figures were not apparent. The tumor infiltrated into the surrounding tissue and entrapped adipose tissue and peripheral nerves. The nodule showed alternating areas of hypercellularity and moderate cellularity and consisted of round to polygonal tumor cells with abundant eosinophilic cytoplasm, which are cells showing epithelioid features (Figure 3C). Although the nuclei of the tumor cells inside the nodule were enlarged, they did not show sufficient atypia to be diagnosed as malignant (Figure 3D). Only a few mitotic figures were identified when the whole nodule was searched.

Microscopic findings of the tumor. D), F) and H) are inside the nodule shown in B). The upper half of D), F) and H) shows consistency with the area of moderate cellularity, and the lower half with that of hypercellularity. A) Proliferating spindle-shaped cells in a background of large and small blood vessels (HE, ×40). B) A nodule present in the tumor showing alternate areas of hypercellularity and moderate cellularity. C) Higher magnification showing sparse spindle-shaped cells with bland nuclei (HE, ×400). D) Both areas inside the nodule are composed of epithelioid cells with abundant eosinophilic cytoplasm. Nuclear enlargement is observed, but mitotic figures are not apparent. E) Spindle-shaped cells showing positivity for desmin (×400). F) Epithelioid cells showing positivity for desmin (×400). G) Spindle-shaped cells showing positivity for progesterone receptors (×400). H) Epithelioid cells showing positivity for progesterone receptors (×400).
Results of the immunohistochemical study in both areas were the same, and the results were positive for desmin (Figure 3E,F), αSMA, estrogen receptors, and progesterone receptors (Figure 3G,H) and negative for AE1/AE3, EMA, S100, CD34, HMB45, and Melan A. The MIB-1 labeling index was less than 1% in most areas of the tumor and 5.8% (58 positive cells per 1000 tumor cells) in the nodule when counting cells with more than moderate nuclear positivity. On the basis of the macroscopic, microscopic, and immunohistochemical findings, this case was diagnosed as AAM with a cellular nodule showing epithelioid features. The cellular nodule was considered benign judging from its degree of nuclear atypia, inconspicuous mitotic figures, and the MIB-1 labeling index.
Discussion and Conclusions
AAMs are rare, slow-growing tumors with a high recurrence rate ranging from 25% to 47%,2,4,5 and they have propensity to occur almost exclusively in the pelvic and perineal region. 6 The high recurrence rate is due to the infiltrative growth of AAMs. Complete surgical resection of the tumor is the primary treatment, and a postoperative follow-up is necessary. In this case, the surgical margin was negative and no recurrence was observed 1 year after operation. Hormonal therapy using gonadotropin-releasing hormones has been used as an alternative treatment for achieving the resolution of AMMs.6,7
The differential diagnosis of AAM includes angiomyofibroblastoma, cellular angiofibroma, superficial angiomyxoma, fibroepithelial stromal polyps, and myxoid leiomyoma. 6 Of these, the most important lesion is angiomyofibroblastoma, which is a recently described, benign, myxoid, and vascular soft tissue tumor of the vulva. In the original description, angiomyofibroblastomas located in the superficial soft tissue and they were usually smaller than 5 cm, and well demarcated. These features contrast with the larger size (often >10 cm) and infiltrative characteristics of AAMs. 8
Histopathological examination reveals angiomyofibroblastomas contain hypocellular and perivascular hypercellular areas composed of bland mesenchymal cells that appear more plump or epithelioid than those of AAMs. As with AAMs, mitotic figures are not easily detected. 8 The recurrence rate for angiomyofibroblastomas is reported to be much lower than that for AAMs. 9 Cellular angiofibromas are much more recently described uncommon mesenchymal tumors with benign nature occurring mainly in the genital region. 10 They are commonly well delineated, situated in the superficial soft tissue, and consist of bland spindle-shaped cells arranged without any characteristic pattern. 10 They are not as large as AAMs, and their size was reported to range from 1 to 9 cm in a recent study. 11
The histopathological findings of our case displayed typical morphology in most areas of the tumor, but the presence of a cellular nodule inside AAM was an unusual finding. In both areas, typical immunohistochemical expression patterns were observed; positivity was observed for demin, αSMA, estrogen receptors, and progesterone receptors. Hormone receptor expression is considered a characteristic feature of AAMs. 6 However, it is also detected in angiomyofibroblastomas and cellular angiofibromas.12,13
Recently, the presence of the high mobility group A (