
Abstract
Cystic nephroma (CN) is an uncommon, benign lesion of the kidney, whose clinical presentation is nonspecific with symptoms such as flack pain, hematuria and urinary tract infection. There are two peaks in the incidence of the tumor, with a bimodal distribution presenting in children between three months and two years, and in adults over 30-years of age. We report a case of CN in the middle part of the left kidney in a 66-year-old male that presented with a singular unilocular, well-circumscribed cyst containing numerous calcifications on the walls and with unremarkable thin or relatively thicker septa from the border with the renal parenchyma, but no solid components. Laparoscopic nephrectomy was performed. Images, histopathological and immunohistochemical features, that are potentially useful for refining this lesion, are discussed.
Introduction
Cystic Nephroma (CN) is an uncommon, benign lesion of the kidney. Its etiology is uncertain and histogenesis is debatable. This tumor has been described in the past with a variety of names such as multilocular cystic tumor, renal multilocular cyst, multiplocular cystic nephroma, renal cystadenoma and partial polycistic kidney,1,2 and it was considered to be a developmental lesion with malignant potential. Approximately 200 cases of CN have been described in the literature to data, 3 with the first original report in 1892 by Edmunds. 4 He described a case of CN of the kidney, which was removed from an 18-year-old girl.
Recent advances in diagnostic imaging have been made in an increased awareness of this type of renal tumor. 5 At the time, surgical intervention is the effective method to exclude malignant cystic lesions of kidney. However, nephron-sparing surgery can be an option depending on the site and size of the lesion. 6 We report an unusual case of a 66-year-old man, who was incidentally diagnosed an unusual presentation of CN while investigating urinary infection.
Case Report
A 66-year old man visited our Department of Urology with a history of dysuria, urinary frequency and recent episode of urinary tract infection. Patient's medical history included hypertension, type 2 diabetes and appendectomy 50 years before. The patient referred a recent episode of urinary tract infection due to
Physical examination was unremarkable except for a mild knocking pain in the left kidney area. Laboratory findings were within normal limits, excepting for microscopic hematuria. Urine cytology was negative for malignancy. He underwent abdominal ultrasound (US) in order to investigate possible cause of recurrence of urinary infection. The results of US demonstrated a well-demarcated cystic mass of the left kidney (about 4 cm in max. diameter) with thickened walls and hyperechoic appearance as large calcifications which occupied the middle part of the kidney. Computed tomography (CT) showed a 4.2×2.6 cm, unilocular, well-circumscribed cyst containing numerous calcifications on the walls and with unremarkable thin or relatively thicker septa from the border with the renal parenchyma, but no solid components. An enhanced CT scan showed a poorly enhancing cystic lesion protruding into sinus (Figure 1). Non-enhanced, cortical phase, and nephrographic phase CT attenuation measurements were 13.0, 15.1, and 24.4 HU, respectively. The renal cystic lesion had features suggestive of malignancy and was classified according to a scheme described by Bosniak as type III.
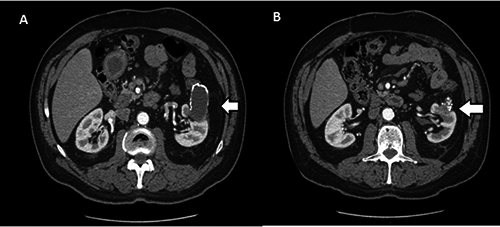
A) Computed tomography (CT) shows a 4.2×2.6 cm, unilocular, well-circumscribed cyst containing numerous calcifications on the walls; B) an enhanced CT scan showed a poorly enhancing cystic lesion protruding into sinus.
The mass was compressing the calycle system and vascular structures at hilum, but no peripheral invasion or distant metastases were detected. Based on the clinical and radiological findings, laparoscopic nephrectomy was performed to remove the tumor. Macroscopic examination revealed a cystic mass, originated from the middle and upper part of the left kidney, with walls of hard consistency, and the maximum thickness of 4mm, screeching to cutting (Figure 2). Microscopically the cyst was lined by a single layer flattened and several calcified areas. The cyst epithelial cells were strongly positive for keratin and epithelial membrane antigen but negative for F VIII, CD34, and vimentin. The septa were composed mainly of mature, predominantly collagenous fibrous tissue and contained dilated vessels. The final histopathological diagnosis was adult cystic nephroma. The patient was discharged 5 days after the operation. The vascular, ureteral, renal pelvis and capsular surgical margins were intact.

Macroscopic examination revealed a cystic mass, originated from the middle and upper part of the left kidney, with walls of hard consistency.
Discussion
Cystic nephroma usually presents as an asymptomatic abdominal swelling, often found during a routine examination. These tumors comprise approximately 1-2% of all renal tumors. 7 CN has a bimodal distribution with two-thirds of tumors presenting in children between three months and two years, with male predominance and second peak in adults over 30-years of age, with a female predominance. Only 5% of this rare tumor is seen in the 5-30 years age-group. 8
There are numerous proposed theories indicating its etiology as a developmental deect. 9 It has also been postulated that it could be neoplastic in origin, probably arising from the ureteral bud. 9 Some authors described ciliar and microvillar appearance of epithelium in electron microscopy and linked this fact with similar aspects of the collecting tubules. 10 Joshi and Beckwith proposed a connection between CN, nephroblastoma and cystic partially differentiated nephroblastoma; however, they empathized the absence of immature tissue in the histological appearance of the tumor. 11
Steele
Conclusions
The present case has been singular for both age of onset and a CN unusual presentation since it was a single cyst with calcified walls and small locules separated by thin septa on the bottom of it. CN is an uncommon cystic lesion of the kidney and should be considered in the differential diagnosis of malignant cystic renal tumors in both children and adults. The combination of clinical, biochemical and radiological features may help in lesion characterization, but only histology can provide the definite diagnosis.