
Abstract
Human T-cell lymphoma virus (HTLV)-associated adult T-cell leukemia lymphoma is a rare cancer in the United States, but there are several areas around the world where the virus is endemic. HTLV-associated adult T-cell leukemia lymphoma has been associated with leukemic arthropathy. We present a patient with HTLV-associated adult T-cell leukemia lymphoma with leukemic arthropathy. Although non-steroidal anti-inflammatory drugs and chemotherapy are often used for treatment, we describe the successful use of radiation therapy in the palliative relief of symptoms from leukemic arthropathy.
Introduction
Human T-cell lymphoma virus type 1 (HTLV-1) was the first retrovirus discovered. 1 This virus is endemic to several areas including: southwestern Japan, the Caribbean, inter-tropical Africa, the Middle East, South America, and Papua New Guinea.2,3 It can cause two different diseases, adult T-cell leukemia lymphoma (ATL) and HTLV-1-associated myelopathy-tropical spastic paraparesis. 3 The former, ATL, is a malignant condition affecting the patient described in this case, whereas, the latter is an inflammatory central nervous system (CNS) condition. There are four subtypes of ATL, which differ in clinical presentation and prognosis: acute and lymphoma, the more aggressive subtypes, and smoldering and chronic, the more indolent subtypes.2,3 The patient was ultimately diagnosed with HTLV associated Acute ATL presentation with organomegaly, lymphadenopathy, an elevated lactate dehydrogenase (LDH) level, and circulating malignant cells, and hypercalcemia, with opportunistic pulmonary infections in a minority of cases as well.4,5 Approximately 10-20 million people are currently infected by the HTLV virus.3,6 The estimated risk of any of these individuals with the virus developing a HTLV-associated malignancy ranges from 5% to 7.6%.3,6,7 The diagnosis of HTLV-associated ATL is made by obtaining a biopsy of the tumor and confirming the presence of HTLV-1 by PCR testing. 8
Here within, we present an interesting case of HTVL-associated ATL in a patient who developed leukemic arthropathy. Though there are no incidences recorded for arthropathy in HTLV associated leukemic. The incidence of articular symptoms in acute leukemia patients as a whole is 4% in adults and 14% in children. 9 This paper is one of only a few that have recorded the use of radiation for palliative treatment of leukemic arthropathy. 10
Case Report
A 41-year-old gentleman from the Caribbean presented with fatigue, joint pain and pruritus of the upper extremity, which eventually progressed to an erythematous skin rash with associated nodularity. He underwent a biopsy of a nodule on the left forearm. The biopsy showed ALK (anaplastic lymphoma kinase) negative, (Classification Determinant) CD 30 positive T-cell lymphoma. PCR testing was positive for HTLV-1. Pathology review revealed large lymphocytes mostly in the perivascular region. The immunophenotypic profile was positive for CD2, CD3, CD4, CD5, CD 25, CD30 (partial), CD43, FOXP3 (forkhead box P3) and T-cell receptor (TCR) beta F1. The tumor cells were negative for all other antigens including: CD7, CD8, CD20, CD56, TCR gamma/delta and TIA-1 (T cell intracellular antigen). These findings supported the diagnosis of a malignant lymphoma of T-cell origin, specifically HTLV-1 associated adult T-cell leukemia lymphoma.
A limited initial staging evaluation done at an outside institution included a bone marrow aspirate and biopsy, which was negative for malignant cells. It is unknown whether additional imaging or laboratory evaluation was obtained initially. The patient was started on Zidovudine plus interferon for presumed smoldering HTLV-1 associated leukemia lymphoma. Clinically, he noted improvement of the skin lesions. However, the pruritus and joint pain persisted, though the symptoms had improved dramatically from initial presentation. Seven months after diagnosis, he achieved a near complete remission. Four months after achieving remission, he had rapid progression of symptoms including bone pain, joint pain, and generalized weakness. Re-evaluation with a PET-CT scan showed multiple sites of lymphadenopathy including: bilateral axillae, hila, peripancreatic, and mesenteric lymph nodes. At the time of recurrence, the patient's presentation was more suggestive of acute HTLV-1 associated adult T-cell leukemia lymphoma. The patient was started on hyper-CVAD chemotherapy (hyperfractionated of cyclophosphamide, vincristine, adriamycin, and dexamethasone). There was significant improvement in the subcutaneous nodules; however, the disease subsequently relapsed again. Despite additional courses of chemotherapy including CHOP (cyclophosphamide, hydroxydaunorubicin, oncovin, prednisone) and ICE (ifosfamide, carboplatin, etoposide), the disease continued to progress with worsening joint pain and enlarging subcutaneous nodules. He was referred to radiation oncology for evaluation of palliative radiation by his hematologist. The patient had the following symptoms before 1st radiation treatment: swelling and inflammation of joints of the upper extremities and nodularity of this region. He also had decreased mobility of his upper extremities. Lower exetremities showed inflammation and nodulatory from the knees to the toes. He also had subcutaneous nodules around his nose and lips. He had lost a significant amount of weight and had difficulty eating now due to mouth/lip sores. A PET/CT two days before starting radiation treatment showed increased activity and thickening of the joint capsules of the hands, elbows, shoulders, knees, and feet, as seen in Figure 1A. He underwent palliative radiation therapy receiving a total of 2400 cGray [(cGy) the SI unit of absorbed radiation dose. One gray equals the energy equivalent of 1 J/kg of matter; 1 Gy equals 100 rad, 1 cGy equals 1 rad] in 8 fractions (300 cGy per fraction) to his bilateral feet, bilateral knees, and bilateral arms (shoulders thru fingers) over seven days. Before radiation treatment, his pain ranged from 4-8/10 on the pain scale. Immediately after his last treatment, his pain scale stabilized at 4/10 and his mobility improved significantly. Two weeks later, he developed ulcerations on his bilateral hands with increased pain in his hands (7/10). Symptomatic management with vinegar soaking technique and oral oxycodone was prescribed. Over the next three months, the ulcers healed and his pain improved. A second PET/CT was done one month after this first radiation therapy to extremities and showed increasing adenopathy and hypermetabolic activity involving the bilateral axilla and inguinal regions, though also showed decreased signal intensity in the joints of extremities. A third PET/CT was done one month from the last PET/CT, this third PET/CT showed significant decrease in signal in all major joints, as seen in Figure 1B. The patient underwent a second course of radiation therapy 4 months after first treatment; this time radiation was given to the bilateral axilla, groin, and hands, receiving 400 cGy in 2 fractions in one day. Clinically, there was a dramatic reduction in the size of the lymph nodes in both the axillae and inguinal region that were palpably tender prior to this 2nd radiation treatment. In addition, his self-reported pain score decreased from 10/10 before the 2nd radiation treatment in his hands and axilla to 0/10.

A) Positron emission tomography (PET) scan two days before the start of first round of radiation treatment, showing increased radiotracer uptake in all major joints. B) PET scan 13 weeks after radiation treatment to his arms, knees and ankles and 4 weeks before the second radiation treatment to his hands, axilla, and groin. This showed significant decrease in radiotracer uptake in several joints.
Two months after 2nd radiation treatment, CT of the chest revealed new bilateral patchy opacities, most prominent in the upper right and left lobes of the lung. Associated symptoms included development of a persistent cough. A bronchial alveolar lavage revealed T-cell leukemia lymphoma. The patient received radiation therapy to the lungs receiving 400 cGy in 2 fractions in one day. His cough resolved following radiation treatment and he continued with additional chemotherapy. Given the very low dose employed for the last two rounds of therapy, treatment was delivered with parallel-opposed beams to areas of symptomatic involvement as identified by physical exam and PET Scan. The patient ultimately passed away two months later due to acute respiratory distress syndrome complicated by sepsis and renal failure.
Discussion
Leukemic arthritis occurs more often in acute leukemia versus chronic leukemia and is more commonly seen in children versus adults. 11 It is typically symmetrical, occurs in multiple joints, with a propensity for the large joints of the body, and often causes pain out of proportion for the amount of inflammation detected. 11 Leukemic arthritis can present as the first sign of leukemia or as a sign of relapse. 11 The incidence of leukemic arthritis ranges from 1.55% to 13.8%. 11 The cause of leukemic infiltration of the joint has been hypothesized as direct hematogenous spread of the cancer to the capsule.11,12 It can be difficult to determine the difference clinically between rheumatoid arthritis and leukemic arthritis. Authors have suggested that aspiration or biopsy of virus infected CD4+ cells from the joint is the main way of differentiation.13,14 Non-steroidal anti-inflammatory drugs (NSAIDs) have typically been ineffective in the treatment of leukemic arthritis. 7 When arthritis is not relieved by NSAIDs and only after adding chemotherapy this helps support the diagnosis of Leukemic arthritis and therefore use of NSAIDs is semi-diagnostic. 11 Table 1 lists several case series using a range of treatments including: NSAIDs, chemotherapy, and radiation in the treatment of leukemic arthritis.10–12,14–18 The cases series were found by searching for reports of leukemic arthritis in PubMed and then filtering for papers with treatments given. Unfortunately, in our patient, the joint pain persisted despite several rounds of chemotherapy. Radiation therapy can be used to treat leukemic arthropathy; however, very little literature exists regarding the effects of radiation on leukemic arthritis.
Summary of leukemic arthropathy cases, respective treatments, and response to treatment.
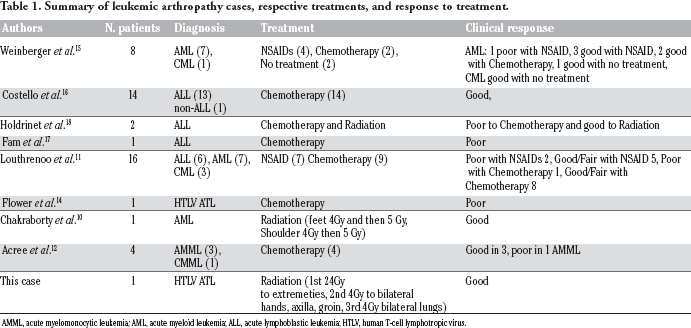
AMML, acute myelomonocytic leukemia; AML, acute myeloid leukemia; ALL, acute lymphoblastic leukemia; HTLV, human T-cell lymphotropic virus.
Chakraborty et al. described a case of an elderly lady with acute myeloid leukemia (AML) who developed severe bilateral ankle pain and left shoulder pain (10/10) with limited mobility. 10 After little relief with chemotherapy, she underwent radiation to the following areas: right ankle (4 Gy in first round and then a second round of 5 Gy), left ankle (one dose 4 Gy), left shoulder (one 4 Gy treatment and then one 5 Gy treatment).14,15 The patient's pain after radiation treatment was 0/10 and she regained mobility l.10,16 We experienced similar results with our patient who had improvement both clinically with decreased pain/improved mobility and radiographically on PET/CT. To our knowledge only one paper exists describing the effectiveness of modern radiation therapy in the treatment of HTLV-associated adult T-cell leukemia lymphoma. 19 Simone et al. reported 10 patients with various subtypes of ATL (acute, smoldering, lymphoma) who underwent treatment to 20 different lesions with radiation therapy (mean dose 35.4/2-3 Gy per fraction, range 12-60 Gy). Following treatment, all lesions responded clinically and radiographically with a 40% complete response after a mean follow up of 9 months. 19 The case series by Simone et al. is in agreement with the result of our case report, in that it suggests radiation therapy is effective in treating HTLV-associated adult T-cell leukemia lymphoma. In this case report also shows relief of leukemic arthropathy. Although the appropriate dose is not clear, our case suggests these patients respond well to lower doses of radiation. For palliation of low volume, low grade non-Hodgkin's Lymphoma, 4 Gy delivered in 2 fractions has been proven effective and can permit multiple courses of therapy without significant risk of toxicity from cumulative doses over time. 20
Conclusions
Human T-cell lymphoma virus-associated adult T-cell leukemia lymphoma is a rare cancer in the US, but on a global scale it is a disease that affects thousands of people. As this patient and others have shown, radiation therapy is effective for palliation of HTLV-associated ATL leukemic arthropathy. Additional research into optimal dosage of radiation for palliation would be beneficial for future patients.