
Abstract
Phyllodes tumors of the breast account for less than 0.5% of breast cancers and present most commonly in women 45 to 49 years old. The importance in managing fibroepithelial lesions lies in distinguishing fibroadenomas, which are benign, from phyllodes tumors, which can be malignant and require complete surgical excision. We report the case of a 56-year-old female who presented with a rapidly enlarging mass in her right breast 18 cm in maximum dimension that completely effaced the breast and distorted the nipple. The patient underwent a successful total mastectomy after core biopsy revealed a diagnosis of phyllodes tumor. Surgical resection is the primary treatment modality; neoadjuvant and adjuvant therapies remain controversial. Here, we report the case of a large malignant phyllodes tumor metastatic to the lungs, review the literature, and discuss diagnostic modalities and adjunct nonsurgical therapies.
Introduction
Phyllodes tumors (PT) of the breast are uncommon fibroepithelial lesions, accounting for less than 0.5% of breast cancers.1,2 Most of them are indistinguishable from benign fibroadenomas and present as smooth, painless breast lumps. In contrast to benign breast lesions, PTs can display a range of biologic behavior including passive behavior similar to fibroadenomas, borderline behavior with local recurrence risks, and malignant behavior with metastatic potential. 2 The metastatic and malignant potential of PTs underscores the importance of distinguishing PTs from fibroadenomas and should be suspected when a patient presents with a large breast mass, a rapidly growing mass, or the patient has a history of prior PT. Breast imaging identifies primary PTs as solid, hypoechoic masses frequently indistinguishable from fibroadenomas, and those that contain cystic areas should raise the suspicion for PT. 3
Core needle biopsy is recommended for initial diagnosis and primarily to differentiate between phyllodes tumor and fibroadenoma. Sub-classification of PTs as benign, borderline, or malignant based on stromal overgrowth, increased stromal cellularity and pleomorphism, and the number of stromal mitoses on a core biopsy is not easily achieved due to limited tumor sampling. Thus, core needle biopsy diagnosis of PTs is associated with a high false negative rate and excisional biopsy is usually required to make a definitive diagnosis.4–6 Histopathologic analysis reveals the characteristic appearance of leaf-like architecture that consists of long, cleft-like spaces and papillary projections of hyperplastic or atypical epithelial-lined cellular stroma, increased stromal overgrowth and mitoses consistently predicting malignant and metastatic potential.2,7
Treatment for PTs is primarily surgical, with current guidelines indicating excisional biopsy or partial mastectomy for tumors less than 5 cm in greatest diameter and total mastectomy for those greater than 5 cm.8–10 Axillary nodal sampling is not required because lymph node involvement is very rare, even in the case of large, malignant tumors.11,12 Approximately 20% of PTs are considered
Case Report
A 56-year-old woman presented in February 2013 with a large breast mass that exhibited skin changes and had significantly increased in size over the past 4 months. Her past medical history was significant for hypertension, high cholesterol, and arthritis of the right knee. Her past surgical history revealed a hysterectomy at age 42 and two cesarean section deliveries. There was no family history of breast cancer. Menarche was at age 9 and she was a gravida 6, para 4.
On physical examination, our patient was a well-developed, well-nourished female with an obvious right breast mass. At the time of presentation the mass measured 18 cm in greatest dimension. The skin was bright blue, although still viable, and was stretched over the mass such that it was difficult to distinguish the nipple from other areas of skin. At the time of surgery, her nipple-areolar complex became grossly necrotic (Figure 1). No axillary, mediastinal, or clavicular lymphadenopathy was appreciated and the contralateral breast was grossly normal.

Pre-surgical photograph of the large phyllodes tumor effacing the right breast and demonstrating skin stretching, vein expansion, and near-total necrosis of the nippleareolar complex.
Ultrasound examination of the right breast revealed a large, lobulated solid mass that was hypoechoic and involved the entire central right breast. Cystic components were identified. There was associated skin thickening anteriorly and internal vascularity was noted within the mass.
Ultrasound-guided core needle biopsy identified a phyllodes tumor with areas of ischemic necrosis and focal squamous metaplasia of the ductal epithelium. The stroma was moderately cellular with mild-to-moderate nuclear pleomorphism. The stromal mitoses varied from 5 to 6 per 10 high power fields (Figure 2A,B). As per the current guidelines, the tumor was interpreted as at least a borderline PT. 15
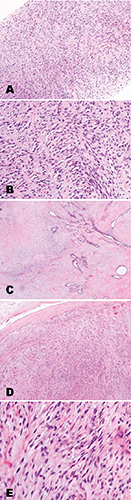
Ultrasound-guided core needle biopsy demonstrating phyllodes tumor with a cellular spindle cell tumor and stromal overgrowth. A) Low magnification of Hematoxylin and Eosin (H&E) stain. B) High magnification of H&E stain. C-E). Histological analysis of surgical specimen. C) Low magnification of H&E stain of the tumor showing variegated stromal cellularity with slit like spaces composed of benign ductal elements. D) Medium magnification of H&E stain showing that the border of the tumor is well-circumscribed. E) High magnification of H&E stain demonstrating hypercellular stroma.
Computed tomography (CT) scan of the chest at the time of diagnosis did not reveal any pulmonary metastatic disease or any other significant findings in the abdomen. Thoracic nodal basins were unremarkable, suggesting that the patient was free of grossly metastatic disease upon presentation.
A standard right total mastectomy was performed excising all thinned skin out of concern for viability. The pectoralis fascia was also removed. Extensive vascularity was noted throughout the tumor, although all bleeding vessels were easily managed with standard techniques. No invasion of the pectoralis muscles or axillary lymphadenopathy was noted at the time of surgery. No axillary nodal sampling was performed. The wound was irrigated and a #19 round Blake drain was inserted in the anterior axillary line, followed by closure of the incision with absorbable suture.
Gross examination of the mastectomy specimen revealed a 22×15 cm firm, rubbery, and well-circumscribed tan mass with areas of hemorrhage and necrosis. Microscopic examination identified a fibroepithelial tumor with prominent stromal overgrowth, hypercellular stroma, and multifocal tumor necrosis admixed with hyaline and myxoid degeneration. Stromal cells showed moderate cytologic atypia with increased mitoses – up to 20 per 10 high power fields, consistent with a diagnosis of malignant phyllodes tumor (Figure 2C-E). All surgical margins were negative.
The patient underwent adjuvant radiotherapy. She remained progression-free until an interval chest X-ray and subsequent chest CT performed one year after surgical resection identified multiple pulmonary nodules that were consistent with metastatic disease (Figure 3A). She had no evidence of chest wall or skin recurrence. Five lesions were detected in the right lung and six in the left. A CT-guided core needle biopsy of a lung nodule identified metastatic phyllodes tumor (Figure 3B,C). At the time of this report, the patient declined chemotherapeutic intervention and is receiving palliative treatment.

Phyllodes tumor metastases to the lung. A) Chest computed tomography (CT) showing multiple pulmonary nodules. B,C) CT-guided biopsy specimen (Hematoxylin and Eosin) of a lung nodule showing metastatic spindle cell tumor morphologically identical to the malignant phyllodes tumor.
Discussion
Phyllodes tumors are rare biphasic breast tumors consisting of epithelial and stromal components, with the latter representing the neoplastic process.4,5 The classic presentation is indistinguishable from fibroadenoma as patients present with a firm, mobile, well-defined, lobulated, and painless mass. 6 Similarly, no pathognomonic features are apparent on mammography or ultrasound so the differentiation between fibroadenoma and PT must be made histologically following tissue biopsy.4,6,7 Current research suggests that MRI may be useful in differentiating PT from fibroadenoma based on the presence of lobulation, cystic components, and heterogeneity on delayed-phase contrast-enhanced T1-weighted imaging. 16 Early identification is of utmost importance in order to prevent the development of giant, malignant, and ultimately metastatic tumors such as the one described in the preceding case report. Preoperative core needle biopsy has a sensitivity of 75% in separating PT from fibroadenoma, therefore, any solid mass that was previously deemed benign but subsequently became symptomatic or exhibited rapid growth would necessitate excisional biopsy.4–6
Several reports indicate that adjunct immunohistochemical analysis of MIB-1 (Ki-67), p53, and p63 may improve diagnostic accuracy, but the expression of those and various other tumor markers has failed to predict outcomes.17–19 Most recently, expression of CD117 (KIT) was shown to be associated with unfavorable pathologic criteria and worse prognosis in patients with PT, although no mutations in the
Nonsurgical therapies for PTs remain controversial and uncertain. Current guidelines from the National Comprehensive Cancer Network (NCCN) indicate that malignant PTs be treated as sarcomas rather than typical breast carcinomas, although no randomized studies of adjuvant chemotherapy currently exist. 22 An observational study followed 28 patients with PTs assigned to either doxorubicin plus dacarbazine or observation alone following surgical resection; this study did not identify any difference in relapse-free survival between the two groups. 23 Due to the general insensitivity of most advanced sarcomas to chemotherapy agents, it is unlikely that chemotherapeutic combination treatment will significantly decrease the rate of relapse or improve survival. Neoadjuvant treatment was reported in one isolated case, with the patient demonstrating no response after three cycles of doxorubicin prior to surgical resection. 24 Emphasis is being placed on the development of patient-specific targeted agents. Whole genome array-based comparative genome hybridization performed on a resected malignant PTs identified an activating mutation in the NRAS gene with concomitant activation of the downstream PI3K/Akt/mTOR pathway. 25 Based on this research, the Ras pathway may play a critical role in the oncogenicity of PTs and therapeutic exploitation of this pathway may prove beneficial.
A prior report identified a use for adjuvant radiotherapy following surgical resection of PTs. 26 In fact, the NCCN suggests radiation therapy for local recurrence, although this is controversial. 22 Radiation therapy can be offered in the setting where further recurrence may cause significant morbidity. 22 Based on statistics from the National Cancer Database, adjuvant radiotherapy for PTs doubled between the years 1998 and 2009, and it was discovered that radiation significantly reduced local recurrence, but had no effect on disease-free survival or overall survival. 27
Conclusions
The rarity of PTs relative to fibroadenomas makes diagnosis a challenge. Suspicion should be raised when a patient presents with a large mass, a rapidly growing mass, or has a history of prior PT. On breast imaging, PTs may have cystic components but no pathognomonic feature is distinguishable leaving biopsy as the only reliable modality for accurate distinction between PTs and fibroadenomas. PTs are primarily treated with surgical resection to either tumor-free or negative margins. Adjuvant treatment for PTs is currently limited to radiation therapy as chemotherapeutic intervention has consistently proven ineffective while genomic-level research performed on resected phyllodes tumors has the potential to identify novel drug targets in the future.