
Abstract
Chronic shoulder pain can be caused by muscle, bone and joint inflammatory and tumoral lesions; however, chronic shoulder pain secondary to benign vascular tumor called glomus tumor is an extremely rare occurrence. To the best of our knowledge less than 15 cases of chronic shoulder pain have been reported secondary to glomus tumor. Herein we report our experience with a young lady who presented with chronic shoulder pain which turned out to be caused by a soft tissue glomus tumor. This case has also been unique because if its large size (about 5 cm in greatest diameter).
Introduction
Glomus tumor was first described by Wood in 1912, 1 but the correct origin was discovered in 1924 by Masson, who suggested this tumor as hyperplasia of normal glomus body. However, it is now accepted that, glomus tumor is a neoplasm originated from modified smooth muscle cells of glomus body (arteriovenous shunt), specialized for regulation of skin circulation. 2 The normal glomus body is basically an arteriovenous shunt that has thermoregulatory function and regulates skin blood flow.3,4
Glomus tumors are characterized by a triad of temperature sensitivity, severe pain, and localized tenderness. 1
They are most commonly less than 1 cm and located in the upper extremity, specially hand and subungual region. 3 This location with small size is so common that, its presence in other locations causes delayed and misdiagnosis. 4
Herein, we report our experience with a patient with chronic longstanding shoulder pain with no response by several therapeutic modalities, which after surgery, pathologic examination showed glomus tumor of shoulder. To the best of our knowledge less than 15 cases of shoulder glomus tumor has been reported so far in the English literature.
Case Report
A 25-year-old lady presented with long standing chronic shoulder pain. She had this pain since adolescence, and during these years, she had tried every local and systemic treatment such as various kinds of non steroidal anti-inflammatory drugs (NSAIDs), local steroid injections, and physiotherapy sessions. Her pain was described as diffuse, vague and chronic, with no significant limitation of motion. Her pain was worse at night and has caused multiple episodes of sleep interruption during the night.
Physical examination, showed significant tenderness on the clavicle. Laboratory findings including CBC (complete blood count), CRP (C-reactive protein), ESR (Erythrocyte sedimentation rate) and all the biochemical tests were completely unremarkable.
With the clinical impression of musculoskeletal and joint inflammatory disorder, she has received NSAID, with no significant change in the intensity of pain. Then she scheduled for physiotherapy sessions, and starting the first session, caused worsening of the shoulder pain. After that, intra-articular steroid has been injected, but no permanent relief was achieved.
After the failure of these conservative therapies, magnetic resonance imaging (MRI) was performed with GAD. Figure 1A shows the MRI by GAD, which shows a large heterogeneous enhancing mass in supraclavicular area with extension to clivus. Bony parts were unremarkable.
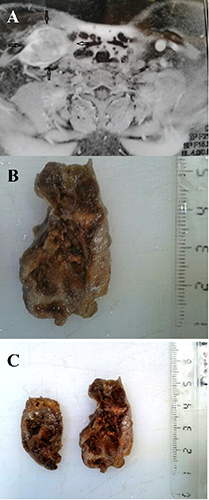
A) Magnetic resonance imaging of the neck with GAD injection shows 49×25 mm heterogeneous mass in the supraclavicular area with extension posterior to the clivus; B) gross of the shoulder mass shows hypervascular brown mass; C) histopathologic sections of the resected mass show monotonous glomus cells with no atypia, no mitosis and no necrosis.
The patient was scheduled for operation and complete excision was performed. During the operation the origin of tumor seemed to be from right supraclavicular region adjacent to periosteum of clavicle.
The specimen received in the pathology lab is shown in Figure 1B. As the figure shows, it was a large tumor with brown color and cystic spaces filled with blood clot.
Histologic sections of the tumor showed small and round uniform cells with indistinct cytoplasmic borders, no mitosis, and no atypia. No necrosis has been identified. With the primary impression of glomus tumor, immunohistochemistry (IHC) was performed. IHC staining showed positive CD31, factor 8 antigen, vimentin and smooth muscle actin (SMA). The cells were negative with cytokeratin, CD99, and leukocyte common antigen (LCA). Ki-67 was very low and less than 1% (Figure 1C).
The tumor was diagnosed as benign glomus tumor, however according to the large size, and deep location, a note was added to the pathology report about the high risk of recurrence and possibility of metastasis.
Discussion
Glomus tumors are true benign neoplasms originated from the glomus bodies, most commonly located in nail bed. 5 This rare tumor represents 1.5% of all benign soft tissue tumors. 3 It seems that glomus tumor has no sex predilection and most common age of presentation has been 20-40 years. 1
Glomus tumor is extremely rare in other locations such as extremities, trunk, and even in viscera.6,7 Forearm is the most common extra digital location and, shoulder and back are the least common sites of involvement by this tumor. 8 Most of the previously reported glomus tumors from various locations in the body have been small with a mean size of 1.9 cm (0.5-4 cm).
The sign and symptoms of this tumor are different according to the location of the involvement, however it usually presents with pain and tenderness.
Because of the small size of the tumor, in locations such as shoulder, palpation cannot be considered as diagnostic modality and our case and previous cases have mostly been diagnosed by imaging studies, mostly by MRI (magnetic resonance imaging). 2 Also, all of the previous cases of glomus tumors in the shoulder area has the experience of different therapeutic modalities before imaging and surgery, such as NSAID and physiotherapy. 2
Table 1 shows some characteristics of the previously reported cases.2,4,5,76,9–18 In the shoulder area, glomus tumor has been reported to be arisen from the bone (such as scapula), 9 muscle (such as deltoid muscle) 10 and soft tissue. 2
Details of the 15 previously reported cases of glomus tumor in the shoulder area.

The diagnosis of the glomus tumor needs pathologic and immunohistochemical confirmation, because these tumors show both vascular (CD31) and muscle (SMA) reactivity. 6 and although histologic features of glomus tumors are very characteristic, however in unusual locations such as shoulder performing IHC (immunohistochemistry) seems to be rational. 1 Another controversial point in this tumor has been criteria of malignancy. 19 Malignant glomus tumor (glamangiosarcoma) has been defined as a glomus tumor with i) deep location and size more than 2 cm, ii) presence of atypical mitotic figures, iii) moderate to high nuclear atypia with 5 or more mitotic figures/50HPF. 20 Our tumor showed no atypia or mitosis, however it has been deeply seated with a large size, so strict follow up will be necessary to identify early recurrence and possibility of metastasis. Now after 6 months of surgery she is completely symptom free with no sign of metastasis.
The treatment of choice for glomus tumors is complete excision and even in malignant counterparts, no chemotherapy or radiation is necessary. 19
Recurrence of glomus tumor in the shoulder has not been reported and all of the previous patients as ours show good response to surgery with no recurrence after follow up between 2 months to 2 years. 7
Conclusions
As a conclusion, although rare, benign vascular tumors such as glomus tumor should be considered in the differential diagnosis of chronic musculoskeletal pains with no response to routine and conventional therapies.