
Abstract
Small bowel cancer is one of the rarest cancers in the gastrointestinal tract. The diagnosis is usually late and most patients presented with the advanced stage. Because of this rarity, there is limited data when making decisions for treatment and biological behavior. Most forms of the cancer occur in the duodenum with surgery being the treatment of choice if the cancer is operable. Chemotherapy has an accepted role in duodenal cancer, with the best form being regimen, which yields the best result in combination with capecitabin and oxaliplatin. Our case patient was present with liver metastasis and a huge mass in her first duodenal region so we were required to use chemotherapy and radiotherapy. Like other duodenal cancers, the metastasis decreased her survival and she died about 13 months after diagnosis.
Introduction
Small bowel cancer is one of the rarest cancers in the gastrointestinal (GI) tract. It comprises of about 70-80% of length and about 90% of the surface area of the alimentary tract. Incidences of small intestine cancers are 40-50 fold lower than that of colon cancers, 1 overall accounting for 1% of GI cancers, 2 with half of them occurring in the duodenum. 3 It seems that duodenal cancer has the worst prognosis than other small bowel carcinoma. Small intestine cancers comprise of 44% carcinoid, 33% adenocarcinoma, 15% lymphoma, and 3 cases of squamous cell carcinoma (SCC) reported. 4 About 45% of these cancers occurred in the 3rd and 4th portion of the small intestine, 3 most of them being sporadic. The most common site of metastasis are the regional lymph nodes, the liver, and the lungs. 5
There are a variety of diagnostic procedures used including barium study, computed tomography (CT) scan, magnetic resonance imaging, entroclysis, entroscopy and endosonography.6–13 Because of a lack of specific symptoms, the diagnosis is usually made late and as a result the overall survival is about 15 months in metastatic patients.14–21 Definitive surgery is the best way to cure. Radical pancreaticodudenectomy (Whipples) operation is the best surgery for the cancers of the first and second parts of the duodenum. There is not any data present to support the benefits of adjuvant treatment after curative surgery, 1 but chemotherapy has an accepted role in the treatment of small intestinal cancers.22–24 The mainstay of chemotherapy regimens are based on SFU. 25 SFU combined with platinum is more effective than SFU alone,26–29 and in some studies, SFU combined with irinotecan or gemcitabine has been useful as well. 16 The best chemotherapy regimen with a 60% response rate and 20% survival rate, however, is a combination of capecitabine and oxaliplation (XELOX). 30 Due to the rarity of these tumors, information about their biology and treatment of this cancer have not yet been completed.31,32
The median overall survival in these patients with metastatic disease was reported at 15 months with a highly active combination of cabcitabine and oxaliplatine. In this article, we reported a case with huge duodenal adenocarcinoma mass with liver metastasis at diagnose.
Case Report
The patient was a 41 years old, non-smoking female who suffered from chronic dyespia, recently complaining of weight loss, nausea, and vomiting. In the physical exam, however, there were no other signs and symptoms recognized except for weight loss. Upper GI endoscopy was done and there was a huge necrotic mass in the first duodenal section which had obliterated the lumen. A biopsy was taken and the result was a poorly differentiated adenocarcinoma with vascular invasion. A CT scan revealed that there was a mass measuring 10.12 cm and multiple liver metastasis yet lab tests showed that renal and liver functions were normal: carcinoembryonic antigen (CEA)=0.34 and hemoglobin=8.5. Because of the liver metastasis, neoadjuvant chemotherapy was done with capecitabine and oxaliplatin and we decided to refer her to surgery if the response to chemotherapy was good. After 4 courses of chemotherapy, we evaluated her with a CT scan with the results showing that the size of the duodenal mass and liver metastasis had increased (12.12) yet chest CT scans and lab tests were normal (CEA=1.46). Due to pain, mass effect, and no response to chemotherapy, we started radiation therapy (RT) with a local field with a total dose of 45 Gy in 25 fractions and there was quickly a dramatic response to radiation therapy. We have CT before and after RT (Figure 1A). Once the pain subsided, we started chemotherapy again with capecitabine and irinotecan and over a 4 course, the mass size was 4.4 cm and the liver metastasis had become smaller (Figure 1B). We referred her for radiofrequency ablation for the liver metastasis and then to the surgery department. Radiofrequency was done but yet the patient was inoperable so we continued chemotherapy with capecitabine and irinotecan for another 2 courses. After seven months of radiation therapy, ascites and peritoneal seeding were happening so we did palliative care for her. Because lab tests were normal and the patient could tolerate further treatment, she received chemotherapy with Gemcitabine along with D1 and D8 every 3 weeks until she died 13 months after the first diagnose.
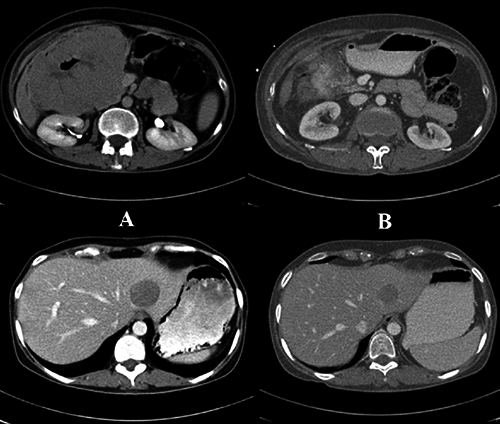
Computed tomography images before (A) and after (B) radiation therapy show the reduction of the liver metastasis.
Discussion and Conclusions
Like other cases of small bowel cancers, in our case, lack of specific symptoms, made the diagnose late. Because she had liver metastasis and a large mass, the diagnose was not difficult. We used CT scan and endoscopy for diagnoses. Most small intestine cancers occur in the 3rd and 4th portions of the duodenum, but in this case, it was in the first duodenal portion. according to previous studies mentioned XELOX as the best regimen for this cancer we started it, but the mass size and liver metastasis increased. We try Capecitabin and irinotecan, it was the best combination in our case. Although the role of neoadjuvant radiation was not well established because of mass effect we had to use it, and the response was deramatic. In multivariate analysis advance stage, poor histological pathology, age and duodenal primary are associated with poor prognosis according to some studies presence of vascular invasion is another factor for poor prognosis. In our case we had vascular invasion, poorly differentiated and duodenal origin. The median survival in patients with metastasis reported 15 months with XELOX. Our patient was alive for 13 months but the best regimen used in this case was capecitabin and irinotecan. Due to the rarity of this tumor, there is not any consensus about treatment. It seems that according to each case we can use surgery, chemotherapy and radiation therapy.