
Abstract
The primary gastrointestinal non-Hodgkin's lymphoma, although rare, is among the most common extra-nodal lymphomas, considering that gastric lymphomas are more common than intestinal lymphomas. Burkitt's lymphoma (BL) is an aggressive form of B-cell lymphoma that is typically endemic in Africa, while non-endemic cases are found in the rest of the world. Primary gastric BL is extremely rare and only around 50 cases have been reported worldwide. Here we present the case of a young HIV-negative male, who was referred to our department with a stage IV gastric BL. He was planned for palliative chemotherapy, but after the first cycle of chemotherapy he succumbed to the progression of the disease.
Introduction
Burkitt's lymphoma (BL) was first described by Denis Burkitt, an Irish surgeon, in the middle of the last century, in Kampala, Central Africa. It was initially believed to be a sarcoma, frequent in children of Tropical Africa.1–3 In 1961, Burkitt met Epstein, an experimental pathologist, who identified a specific virus in the samples of tissues from this lymphoma. The virus became known as Epstein Barr virus (EBV). This was the first time ever that a virus was found to be involved in the pathogenesis of a tumor in humans. In Africa, BL continues to be the most common malignancy in childhood. 4
The World Health Organization (WHO) classification describes three clinical variants of BL, i.e. endemic, sporadic, and immunodeficiency-associated. Endemic BL is seen in African children between 4-7 years of age with a male to female ratio of 2:1. It affects the bones of the jaw and the face, the kidneys, the gastrointestinal tract, the ovaries, the breast, and other extra-nodal sites. 5 The incidence of endemic BL is higher in Africa. 6 Nearly all cases are caused by EBV.
Sporadic BL occurs worldwide. In the U.S. and Western Europe, it accounts for 1-2% of lymphomas in adults and up to 40% of lymphomas in children. 6 The most common sites involved is in the abdomen, especially in the ileocecal area, while the ovaries, the kidneys, the omentum and Waldeyer's ring are other potential affected sites. The central nervous system (CNS) involvement at presentation has been reported in 13-17% of the sporadic cases. 6
Immunodeficiency virus-associated BL occurs mainly in patients infected by HIV. BL accounts for 30-40% of non-Hodgkin's lymphoma in HIV-positive patients.6,7
Case Report
We present the case of a 40-year-old male who came to the outpatient department of our hospital in January 2013 with a 5-day history of melena, dysphagia and abdominal pain. He reported a history of tobacco and alcohol use for the past 20 years and had no other associated comorbidities. On physical examination his Eastern Cooperative Oncology Group (ECOG) performance score was 3 and had associated pallor. The abdominal examination revealed a vague, firm, tender mass with associated ascites.
Proceeding with investigations, the upper gastrointestinal endoscopy revealed an ulceroproliferative tumor extending almost from the cardia down to the antrum of the stomach (Figure 1). Carbohydrate antigen (Ca) 19-9 and carcinoembrionic antigen (CEA) were within normal limits. The PET-CT showed a 16.2×7.3 cm hyper metabolic exophytic soft tissue mass arising from the gastro-esophageal (GE) junction and the lesser curvature of the stomach extending to involve the pancreas and the peri-portal region along with peritoneal deposits (Figure 2). The PET-CT also showed pleural thickening, bilateral pleural effusion, collapsed right lower lobes, patchy infiltrates in bilateral lung, bilateral enlarged internal mammary nodes, deposits in the left lateral chest wall, omental thickening and moderate ascites.

Upper gastrointestinal endoscopic images.
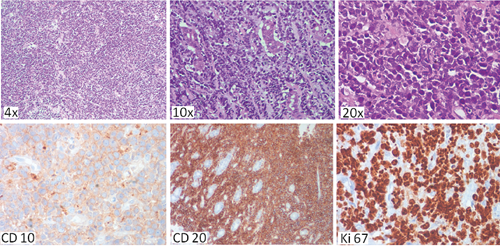
Staining with Hematoxylin and Eosin (upper line). Immunohistochemistry staining (lower line).
A gastric biopsy revealed a diffuse infiltration of the sub-mucosal layer by atypical lymphoid cells having coarse nuclei and indiscernible cytoplasm, arranged in box-like contours (Figure 3). A brisk mitotic activity with apoptotic figures was observed. The immune histochemical evaluation revealed neoplastic cells that were positive for LCA, CD 20, and CD 10 and negative for CK, CD5, CD3, Bcl2 and cyclin D1. M1B1 (Ki 67) proliferation index was 99%. The pleural fluid cytology was positive for malignant cells. The bone marrow aspiration study showed a normo-cellular marrow. He was tested for HIV and was found to be negative. Tests for Helicobacter pylori and EBV were however not carried out.

Positron emission tomography-computed tomography (PET-CT) images: cut sections at the level of stomach lesion. A) CT, cross sectional image. B) PET-CT fusion, cross sectional image. C) PET, cross sectional maximum intensity projection (MIP) image. D) PET, coronal MIP image.
After taking into consideration all the clinical, radiological and pathological findings, a final diagnosis of Burkitt's lymphoma arising from the stomach was made. Due to the poor performance score, rarity and advanced disease stage, the case was discussed in the multidisciplinary clinic and with the family members and it was decided to go ahead with palliative chemotherapy with cyclophosphamide and rituximab. He received 1 cycle of palliative chemotherapy, progressed while on treatment and finally succumbed to the disease in February 2013.
Discussion
The gastrointestinal (GI) tract is one of the most frequent sites of extra-nodal non-Hodgkin's lymphomas (30-50%).8,9 Although secondary GI involvement is relatively common in lymphoma, primary gastrointestinal lymphoma (PGL) is rare. PGL is defined as a lymphoma presenting with symptoms located only or predominantly in the GI tract. 10 Moreover, evaluation, diagnosis, management and prognosis of PGL differ considerably from other extra-nodal lymphomas, and are hence considered as a distinct entity in the literature. The stomach is supposed to be the most frequent site of PGL.11–17 However in a few American and Egyptian studies, the intestine is considered the most common site of PGL.10,18–20
The primary involvement of BL or a small non-cleaved cell lymphoma in the GI tract, although rare, has been reported in the literature. Despite gastric lymphomas being more common than intestinal lymphomas, the primary gastric involvement is extremely rare in BL (Table 1).10–24 The male-to-female ratio ranges from 2.5 to 6.3,19,22 indicating a clear male predominance. Gastrointestinal Burkitt's lymphoma (GI-BL) is found to be more common in the second decade. 17 However the median age varies between 7.9 years and 48 years in various reports.20,25 The etiological relationship between BL and EBV has been well-studied and documented. EBV is associated with 98% of endemic BL, 20% of sporadic cases, and 30-40% of HIV-associated cases. 26 Confirmation of this causal relationship in GIBL has not yet been validated. Studies of sporadic cases have been reported with Helicobacter pylori as causal factor of gastric BL,25,27,28 and eradication of Helicobacter pylori leading to a complete remission of gastric BL.29,30 The association of BL with HIV infection is well-known also in the GI tract. 31 According to a study conducted in India, 50% (3/6) of the gastric BL cases presented an associated HIV infection. 17
Burkitt's lymphoma: summary of previous studies.

BL is considered to be a high-grade lymphoma, which has typically with a rapid progression. It has a growth fraction close to 100% and a doubling time of around 25 hours. 6 Consequently it should always be addressed as a medical emergency. In a case series of 21 cases of gastric BL, 19 stage 1 and 2 were found in five patients per stage, and stage 4 in 11 patients. The body and the antrum of the stomach were the most common sites of involvement. All the cases were treated with intensive systemic chemotherapy and 71% (17/21) of patients achieved a complete response. As to patients in stages 1 and 2, 9/10 showed a complete response. This confirmed once again that early diagnosis and treatment of gastric BL is of utmost importance to ensure remission.
Although BL is one of the first malignancies that showed a complete response to intensive chemotherapy, 32 adult patients particularly at an advanced stage of the disease have a negative prognosis with rapid progression and a high likelihood of CNS metastasis. 33 Initial efforts to treat BL with the usual regimens for NHL failed to show the expected benefits probably due to the high proliferative rate of BL cells which caused the viable tumor cells to recover and re-enter the cell cycle between two chemotherapy cycles. Dose-intensive chemotherapy seems to be the answer to this problem. One of the Indian series reported the use of eight cycles of a dose-intensive MCP 842 protocol to treat all the GI-BL cases.14,34 It must be remembered that the tumor lysis is very common due to the high proliferation rate of the tumor. As a result, precautionary measures need to be taken to prevent the tumor lysis syndrome.
Central nervous system prophylaxis is strongly recommended in almost all studies, as there is a 20-30% lifetime risk of CNS involvement. 35 Prior to the introduction of dose-intensive chemotherapy with CNS prophylaxis, 30-50% patients had a CNS relapse. 26 Hence some form of CNS prophylaxis, such as systemic or intrathecal methotrexate or cytarabine, has been part of all chemotherapy regimens used in BL. The relapse rate decreased to 6-11% with the inclusion of CNS prophylaxis in the existing treatment protocol, with the above mentioned approach. 36
The optimal chemotherapy treatment for GI-BL is largely undefined and is extrapolated from the pediatric literature. Most BL regimens have been evaluated in non-randomized single-center studies, and hence cannot be generalized. The Magrath Protocol with CODOX-M/IVAC regimen was a milestone in the history of chemotherapy for BL. Two cycles of cyclophosphamide, vincristine, doxorubicin, high-dose methotrexate, and intrathecal therapy (CODOX-M) alternating with ifosfamide, etoposide, high-dose cytarabine (IVAC), and intrathecal therapy were used for high-risk BL and three cycles of CODOX-M alone, for patients at low-risk. Both children and adults treated with this regimen had excellent outcomes: the Event Free Survival (EFS) rate at 2 years was 92% for the group as a whole. 37 But unfortunately this was associated with significant toxicity causing for instance myelosuppression, mucositis, neuropathy, and even some treatment-related deaths.6,38 Several centers suggested different modifications of the Magrath Protocol in order to reduce toxicity. The Dana-Farber Cancer Institute used a different dose of fractionated cyclophosphamide and vincristine, but with a higher dose of doxorubicin. They found no treatment related deaths, no severe neurotoxicity and only one case of severe mucositis. The 2-year EFS rate was 64% for all patients, 100% for low-risk patients, and 60% for high-risk patients.37,39
Similarly, the United Kingdom Lymphoma Group also made a few modifications to the same protocol achieving a 2-year overall and EFS rate of 73% and 65% respectively (82% and 83% in the low-risk group and 70% and 60% in the high-risk group respectively).37,40
Since BL involves a significant expression of CD20 on the surface and rituximab is a monoclonal anti-CD20 antibody, the introduction of this drug in the existing chemotherapy protocols was thought to improve the outcome of BL patients. According to a small series from M.D. Anderson cancer center, a complete remission rate of 89% was achieved when rituximab was used in an hyper-fractionated regimen containing cyclophosphamide, vincristine, doxorubicin, and dexamethasone (hyper-CVAD), along with CNS prophylaxis.37,41
In a recent retrospective analysis by Wildes T.M., it was seen that the addition of rituximab to chemotherapy (R-chemo) improved survival in locally advanced BL with or without CNS involvement. R-chemo was found to be associated with significantly longer overall survival (OS) than with conventional chemotherapy alone (5-year OS 70% and 29%, respectively, P=0.040). In the multivariate regression analysis, a poor performance status and the CNS involvement were associated with poorer survival. 42
Advances in the treatment methods have led to a major improvement in the outcome and survival of BL patients. However, according to a recent survival study by Brown University conducted in 2013, this improvement did not appear in patients at an advanced stage, with an older age and among black patients. 43 This study has developed a novel prognostic scoring system which would help quantify the potential for remission in newly diagnosed adults. In a prospective NILG study, using the German short intensive rituximab-chemotherapy program, excellent OS and DFS rates of 67% (75% for those aged ≤60 years) and 75% (82% for those aged ≤60 years) respectively were achieved. 44 Park analyzed the distinct features, the response to treatment and the outcome of gastric BL and showed that gastric BL at early stages 1 and 2 had an outstanding outcome suggesting that these stages could represent a separate subtype with a distinct biology.
Conclusions
Gastric BL is an uncommon form of non-Hodgkin's lymphoma in adults with a high proliferation rate, aggressive nature and poor prognosis. The optimal therapy for this disease is still unknown and is mainly adapted from pediatric treatment regimens. Aggressive chemotherapy with the addition of rituximab and CNS prophylaxis should be part of all treatment regimens. Advanced stage, older age groups are associated with poorer outcomes. With early diagnosis and prompt appropriate treatment, long-term survival rates of 70-80% may be possible, while a delay in treatment may be lethal to such patients.
Footnotes
Conflict of interests: the authors declare no potential conflict of interests.