
Abstract
Though rarely reported, neoplasms of the clavicle occur, and their symptoms can be mistaken for more common shoulder conditions. We present the case of a benign clavicular neoplasm, rarely seen in adults, presenting with pain, and eventual pathologic fracture in a 49 year-old. A 49 year-old male firefighter underwent arthroscopic rotator cuff repair for shoulder pain after magnetic resonance imaging revealed supraspinatus tendon tear. The patient's pain persisted after surgery, and was described as routine until he developed severe pain after minor blunt trauma. A local Emergency Room performed the first x-rays, which revealed a pathologic fracture of the distal clavicle through a destructive lesion. The patient was referred to an orthopedic oncologist, who performed incisional biopsy, which initially diagnosed osteomyelitis. The patient was subsequently taken to surgery for debridement. Pathology then yielded the diagnosis of eosinophilic granuloma. The patient was taken back to surgery for formal curettage with open reduction and internal fixation. The patient's pain resolved, the pathologic fracture fully healed, and the patient returned to full time work as a firefighter. Though workup for common shoulder conditions often identifies incidental benign lesions of bone, the converse can be true. Persistent pain despite intervention should raise concern for further investigation. An x-ray alone can reveal a destructive bone lesion as the source of shoulder pain.
Introduction
Degenerative conditions of the shoulder are frequently encountered by the orthopedist and thus often described. 1 Neoplasms of the clavicle are less commonly described, but nevertheless occur. Primary clavicular neoplasms are reported to occur in up to one per cent of all primary bone tumors. 2 The addition of secondary malignancies raises this number even higher.3,4 Infection should always be considered in the setting of destructive bone lesions, but is less common in adults without identifiable risk factors. 5 Eosinophilic granuloma presents as a lytic lesion with a predeliction for the flat bones, usually associated with young patients.
Shoulder pain is often attributed to common conditions such as glenohumeral or acromioclavicular arthritis, rotator cuff tendinopathy, bicipital tendonitis, frozen shoulder, and other frequent degenerative conditions. In attempts to alleviate the patient's discomfort, investigation and treatment is often initially directed toward these conditions. Less common, but still applicable, conditions often go overlooked in the initial management of shoulder pain.
Though clavicular neoplasms occur with less frequency than degenerative conditions of the shoulder, any busy orthopedic shoulder specialist will likely see at least one in their career, if not every year. The traditional differential diagnosis for a destructive lesion in a patient over the age of 40 consists of metastatic disease (most commonly), followed by myeloma, and then lymphoma. 6 Though this differential is often correct, it is by no means universal. Other benign, yet destructive, conditions may present. We report the interesting case of a destructive clavicular lesion in an adult, initially diagnosed with and treated as a rotator cuff tear, and then misdiagnosed upon initial biopsy, to demonstrate that i) not all shoulder pain occurs secondary to a degenerative condition, ii) the x-ray is an invaluable initial diagnostic tool, iii) pathology is not always an exact science, iv) eosinophilic granuloma can occur in the adult, and v) not all destructive bone lesions in adults represent metastatic disease.
Case Report
A 49-year-old, right-hand dominant male fireman presented to his sports surgeon with progressive right shoulder pain. Magnetic resonance imaging (MRI) demonstrated a supraspinatus tear, and he underwent arthroscopic rotator cuff repair under regional anesthesia. The patient continued to have pain postoperatively. Six months after surgery, he noted severe shoulder pain after minor blunt trauma, and he sought care at his local ED. X-rays were then taken for the first time, revealing a pathologic fracture through a destructive lesion in the distal right clavicle (Figure 1).
This radiograph reveals the patient's destructive lesion in the right distal clavicle.
The patient was referred to an orthopedic oncologist, where physical exam revealed right distal clavicle swelling and exquisite tenderness to palpation. Serum inflammatory studies were normal (ESR=4, CRP=0.3), and the white blood cells (WBC) count was mildly elevated [WBC=14.1 (81% PMN)]. MRI confirmed no skip lesions, bone scan showed increased uptake in the right clavicle only (Figure 2), and computed tomography (CT) showed pathologic clavicle fracture with no evidence of visceral masses (Figure 3). The patient was taken for incisional biopsy, with histology revealing inflammatory cells and S100 negativity (Figure 4), yielding the diagnosis of acute osteomyelitis. The patient was taken back to surgery for formal irrigation, debridement, and antibiotic bead placement (Figure 5).
This bone scan reveals increased uptake (mineralization) localized to the right clavicle.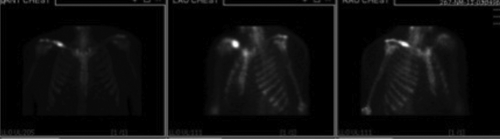
The computed tomography scan reveals a destructive clavicular lesion with associated pathologic fracture.
A) This high power Haematoxylin & Eosin stain reveals histiocytes, lymphocytes, and polymorphonuclear leukocytes amidst hyalinized vesses and a fibrous stroma, consistent with osteomyelitis or hematologic neoplasm; B) this S100 immunostain shows weak positivity or negativity, suggesting against the diagnosis of eosinophilic granuloma.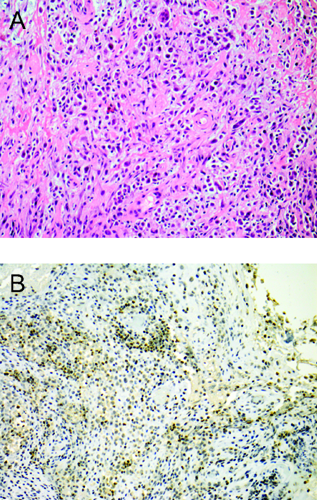
This intraoperative photograph shows the clavicle after I&D and antibiotic bead placement.
Pathology from the latest procedure revealed S-100, CD1a, and Langerin positivity, confirming the diagnosis of eosinophilic granuloma (Figure 6). All cultures remained negative. Skeletal survey and serum LDH were normal. The patient was taken back to surgery for formal curettage with open reduction, internal fixation, and bone grafting (Figure 7). Medical oncology recommended no further local or systemic treatment. The patient's clavicle healed without complication (Figure 8), his pain resolved, and he returned to full work. Surveillance studies have confirmed no locally recurrent or systemic disease 1 year postoperatively.
A) This high power immunostain demonstrates CD1a positivity, favoring the diagnosis of eosinophilic granuloma; B) this high power specialized immunostain displays Langerin positivity, further confirming the diagnosis of eosinophilic granuloma.
A) This intraoperative photograph shows the clavicle after open reduction and internal fixation with bone grafting; B) this intraoperative radiograph of the right clavicle demonstrates the open reduction and internal fixation of the clavicular pathologic fracture.
This radiograph taken 1 year postoperatively shows the healed pathologic fracture with consolidation of the former lesion.
Discussion and Conclusions
We present the case of a middle-aged man who presented to the sports surgeon with shoulder pain. He underwent arthroscopic treatment for his rotator cuff tendonopathy. His pain persisted, but x-rays were never taken until the patient's pain became severe and he sought treatment at his local ED, where a pathologic fracture through a destructive bone lesion was discovered. Incisional biopsy diagnosed acute osteomyelitis, presumed to have been caused by his regional block at the time of arthroscopy. After irrigation and debridement, a second pathologic sample revealed eosinophilic granuloma, which became the final diagnosis. Benign asymptomatic bone lesions (i.e., enchondromas) are often discovered incidentally in the workup of degenerative conditions of the shoulder. In this case, the converse occurred. This case highlights the importance of preoperative collaboration with musculoskeletally trained radiologists, medical oncologists, and pathologists to establish an extensive differential diagnosis prior to sampling. Bone tumors in adults presenting as degenerative or traumatic shoulder conditions have also been described in the literature. In one report, two cases of shoulder girdle osteochondromas (clavicle and acromion) presented with rotator cuff syndrome, relieved by resection.7,8 Clavicular osteoid osteoma has been documented in case reports: one in a wrestler initially diagnosed with an injury, 9 and two presenting as brachial plexopathy. 10 Another series reports shoulder neoplasms initially presenting as adhesive capsulitis, noting that tenderness to palpation was a key distinguishing factor separating tumor from the traditional frozen shoulder. 1 Another case report documents a patient with a 20-year history of shoulder pain secondary to a supraclavicular glomus tumor. 11 An review of an institution's series of 143 bone tumors of the shoulder girdle yielded only one case of eosinophilic granuloma, which occurred in the scapula. 4 Distal clavicular osteolysis, so-called weightlifter's shoulder, presents as painful shoulder with radiographic evidence of bone lysis in the distal end of the clavicle. The condition is more common in middle-aged males who engage in repetitive, stressful shoulder activity, and is thought to result from repeated microtrauma with subchondral stress fracture and associated remodeling. 12 Osteomyelitis of the clavicle following a regional block has not been described in the literature; however, infection of the clavicle following subclavian venipuncture has been documented. 5
After a careful history and physical examination, radiographs are the next most important tool for evaluation of a patient with a bone abnormality.6,13 Given their relative availability, safety, low cost, and high diagnostic yield, plain radiographs should always be obtained in the setting of prolonged joint or extremity pain, and prior to obtaining more extensive imaging (MRI, bone scan, etc.).6,13 In this case, a simple plain radiograph would have identified the lesion prior to pathologic fracture, potentially decreasing patient morbidity.
Diagnostic accuracy of open surgical biopsy ranges from 94 to 100%.14–16 Therefore, up to one in seventeen patients may be misdiagnosed even with open biopsy and even at institutions experienced with bone and soft tissue pathology. One should keep this accuracy in mind when dealing with diagnostic challenges and unusual presentations. This inaccuracy can be mitigated through sampling from all areas of the lesion, frozen section analysis to confirm sampling at the time of biopsy, and repeat sampling at the time of index procedures.
The incidence of primary clavicular bone tumors ranges from 0.45–1.01% of primary bone neoplasms.2,17 Histological pathology of the primary tumors varies, with a majority of case reports revealing myeloma, osteosarcoma, or Ewing's sarcoma.17–19 These studies have also demonstrated that the majority of primary clavicle tumors are malignant,17,10 and malignant histology is correlated with older age (>50 years).3,20 Metastatic lesions to the clavicle rarely occur (2% of shoulder girdle neoplasms), and correlate with advanced age. 4 In the case of malignancy, partial or complete resection of the clavicle without reconstruction is a viable treatment option with minimal functional disability.21,22
Eosinophilic granuloma refers to the non-neoplastic process involving the Langerhans cell, also known as Histiocytosis X or Langerhans cell histiocytosis. The condition predominately effects the flat bones or diaphysis of long bones, and has been documented to occur in 18.5% of primary clavicular lesions. 20 More extensive forms of the disease consist of Hand-Shuller-Christain and Letterer-Siwe diseases, in which the process becomes disseminated and the prognosis worsens. Oncologic textbooks often refer to eosinophilic granuloma as a pediatric disease, with some stating most patients are between 5 and 20 and the disease occur(s) most frequently in children under 15 years of age.23,24 Careful review of the literature shows clearly documented incidences of the disease in the adult population. A study of 32 EG patients documented 47% to be skeletally mature, with these patients ranging from 16 to 28 years of age. 25 These authors concluded that the skeletally mature group experienced a higher rate of recurrence after treatment than the younger counterparts. 25 Kilpatrick et al. reviewed 263 EG cases in the Mayo system, finding 35% of these patients were adults up to 71 years of age. 26 Another well-respected publication cites a 39% incidence in patients over the age of 21. 17
Diagnosis of EG is based upon history, physical examination, plain radiographs, and biopsy. Histology reveals histocytes and eosinophils, which stain positive for S-100, CD1a, and intracellular lysozyme. Electron microscopy may reveal tennis-racquet shaped Birbeck granules, though is infrequently used. Staining may be equivocal, as in our case, highlighting the importance of diverse and repeat sampling upon initial biopsy and subsequent procedures involving destructive lesions. The treatment of osseous EG is controversial, and can consist of biopsy alone, corticosteroid injection, or curettage, with chemotherapy and radiation therapy as adjuvant or solitary treatments.12,17,25,26 Adult EG has been shown to have a higher recurrence rate than the traditional pediatric form, 7 so EG in the skeletally mature may require more aggressive intervention. A recent study from the Rare Cancer Network showed that adults with osseous EG treated with surgery and radiation experienced significantly decreased rate of local recurrence compared with the less comprehensive treatment modalities; they noted that radiation alone for primary treatment was associated with an unacceptable rate of local recurrence (50%) in these adults.12,27
Progressive shoulder pain can be caused by a destructive clavicular lesion which may not be evident within the field of the routine shoulder MRI, but very evident on routine shoulder radiographs; therefore, the radiograph should be the initial imaging study for progressive shoulder pain. A destructive clavicular neoplasm in the adult can be attributed to a variety of causes, ranging from metastatic disease to primary malignancy to benign neoplasm to osteomyelitis; and though considered a pediatric disease, eosinophilic granuloma may be the cause of a destructive bone lesion in an adult. Final pathologic analysis may not always be correct, underscoring the importance of repeat sampling of atypical lesions. The possibility of neoplasm should always be considered in the patient with worsening shoulder pain despite intervention for degenerative disease.