
Abstract
Gastrointestinal stromal tumors are the most common mesenchymal tumors of the gastrointestinal tract. The introduction of a number of small molecule tyrosine kinase inhibitors has revolutionized the management of metastatic disease. Surgery is the mainstay of management for localized disease. Patients with high risk tumors are treated with adjuvant imatinib. We report the rare presentation of a localized primary small bowel gastrointestinal stromal tumor in association with multiple liver abscesses. Cystic liver lesions should be fully evaluated in gastro intestinal tumor patients to exclude an infective cause. Treatment with intravenous antibiotics resulted in clinical and radiological improvement of the liver abscesses. The small bowel tumor was treated with surgical resection.
Introduction
Gastrointestinal stromal tumors (GIST) are the most common mesenchymal neoplasm of the gastrointestinal tract, characterized on immunohistochemistry by expression of CD117 (KIT) which distinguishes it from other spindle cell tumors. 1 Hirota and colleagues discovered that the majority of these tumors harbor an activating mutation in the KIT oncogene, and this has led to significant improvements in understanding the biology of this rare disease and consequently substantial improvements in therapy. 1 GISTs have an incidence of 10-14 cases per million people each year. They can arise in any part of the gastrointestinal tract, but the most common primary sites are the stomach (60%) and small intestine (30%). They usually metastasize to the liver, omentum and peritoneal surfaces.
Surgical resection is the definitive management for localized disease followed by adjuvant imatinib for patients with high risk features. The introduction of small molecule tyrosine kinase inhibitors has revolutionized the management of metastatic GIST. 2 We report the case of a patient with multiple liver abscesses associated with a primary small bowel GIST. The radiological appearances of the liver abscesses could easily have been misinterpreted as metastatic disease.
Case Report
A 31-year old Caucasian man with a history of iron deficiency anemia and intermittent gastrointestinal bleeding over the course of 4 years, presented with cyclic fever, a mild cough, loss of appetite, and occasional diarrhea. The patient had no causes of immunosuppression such as HIV and he was on no medication. Previously, four esophagogastroduodenoscopies, a capsule study and colonoscopy (performed at another institution) found no source for blood loss. It was noted that his hematocrit had fallen from 43 to 33. He was admitted to hospital and commenced on empiric antibiotic therapy with azithromycin.
A CT scan of the thorax, abdomen and pelvis showed a 3×3.5 cm mass in the small bowel and numerous hypodense lesions throughout the liver, measuring up to 2 cm. A PET/CT demonstrated mild FDG uptake in the small bowel mass and intense uptake in the liver lesions (Figure 1). To differentiate liver infection versus malignancy, a CT-guided liver biopsy was performed. It showed necrotic cells, a few polymorphonuclear leukocytes, and purulence, but there were no malignant cells (Figure 2). The gram stain showed no organisms, and the culture was negative. Aspiration of one of the liver lesions showed many cells, but no polymorphonuclear leukocytes and no organisms. The culture from the aspirate was negative for bacteria, fungi, and acid fast bacillus.
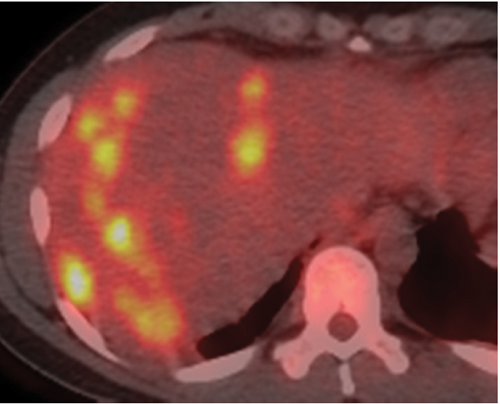
Pre-therapy positron emission tomography/computerized tomography with multiple foci within the liver demonstrating markedly increased FDG uptake.
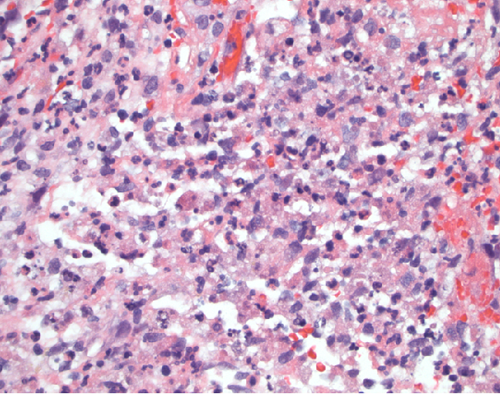
Biopsy of liver parenchyma with a mixed inflammatory infiltrate with an abundance of neutrophils and abscess formation.
The patient continued experiencing febrile episodes on azithromycin, and consequently antibiotic coverage was broadened to metronidazole and ceftriaxone. Due to persistent febrile episodes, his antibiotic treatment was revised to ertapenem, and subsequently to a combination of metronidazole, daptomycin, imipenem and micafungin on the 6th and 8th day post admission, respectively. The patient was transferred to the University of Washington Medical Center and the antibiotic schedule changed to metronidazole, daptomycin, meropenem and caspofungin, as per institutional guidelines. Repeat chest X-ray and blood cultures remained clear during this time. With this therapy, the patient's clinical condition dramatically improved and the febrile episodes completely ceased, indicating the liver lesions were most likely infectious abscess. Blood cultures remained negative and further investigations revealed no cause for the temperature spikes. His ESR was 98 and CRP 265. CEA was undetectable at less than 0.7. With the cyclic fever resolved, the patient was discharged and the treatment was modified to intravenous daptomycin and meropenem.
Two weeks following discharge from hospital, with no further febrile episodes, the patient underwent laparoscopic small bowel resection and core needle biopsy of one of the liver lesions. The small bowel mass was 3 cm in size and located in the distal jejunum. On pathology the small bowel mass had a spindle cell morphology and on immunohistochemistry the tumor cells showed expression of CD117, confirming the diagnosis of a gastrointestinal stromal tumor (Figure 3). The mitotic activity was 0-1 mitosis/10 HPF, no necrosis was seen, and all margins were clear. A follow up FDG-PET/CT a month post surgery showed a near complete resolution of the innumerable hypermetabolic foci scattered throughout both lobes of the liver (Figure 4). Only a single punctate focus of FDG accumulation was identified within the liver with a maximum SUV value of 4.6 which was a substantial decrease in size and maximum SUV in comparison to the previous examination. CT with intravenous contrast showed significantly smaller hypodense lesions scattered throughout the liver. After about 6 weeks of treatment with daptomycin and meropenem, his antibiotic schedule was changed to oral moxifloxacin and augmentin, which were eventually stopped. He was on antibiotic therapy for a total of 12 weeks. The patient has recovered fully and is feeling well 17 months following the laparoscopic small bowel resection. Surveillance scans have shown no evidence of local recurrence or metastatic disease.

Biopsy of small bowel mass with spindle cell morphology, consistent with gastro intestinal stromal tumor.

Post-therapy positron emission tomography/computerized tomography showing complete resolution of the lesions following antibiotic treatment.
Discussion
There are very limited data regarding the association of liver abscesses and primary GIST.3–7 In previous cases, the identified organisms were commensal obligate or facultative anaerobic gram positive organisms: gemellae morbillorum and α-hemolytic streptococcus (Streptococcus milleri and Streptococcus intermedius).4–6 Gemellae morbillorum may be found as part of oropharyngeal normal flora. Streptococcus inhabit various mucous membranes including the oral cavity, oral pharynx, gastrointestinal tract, and genitourinary tract. 8 The proposed mechanism of the infections includes the breakdown of mucosa by the GIST lesions, allowing these organisms to invade and systemically infect the host. Alternatively, it is also possible that the liver metastasis can serve as an underlying pathway for infection. A common cause of pyogenic liver abscess is biliary tract disease and malignancy in the liver. 9 Metastatic disease could potentially physically obstruct the biliary tree, allowing bacterial proliferation. In some cases these infections have initiated a full gastrointestinal workup, revealing the underlying associated asymptomatic malignancies. 10
The initial PET-CT scan showed intense FDG uptake in the liver lesions, consistent with metastatic disease in the liver. Repeated investigations to identify potential causative organisms were negative, and the patient did not initially respond to empiric antibiotic therapy. Based on the FDG-PET appearances, the patient could potentially have commenced systemic therapy with imatinib as treatment for metastatic disease. If the patient had been commenced on empiric imatinib and infection was the cause of the liver lesions, it could have resulted in neutropenia and worsening of his clinical condition. Notably, the mortality rate due to liver abscesses is considerable (19%), 11 and consequently any intervention with the risk of neutropenia would have posed a significant challenge for this patient.
Conclusions
Pyogenic liver abscesses associated with gastro intestinal stromal tumors are rare, but this case clearly highlights that these can easily be misinterpreted as liver metastases. It should be noted that concomitant presentation of primary GIST with fever and liver lesions should be evaluated carefully for liver abscess involvement. Infection should be rigorously excluded prior to the initiation of tyrosine kinase therapy.