
Abstract
The patient was a 62-year-old man diagnosed as having prostatic extra-gastrointestinal stromal tumor (EGIST) who was treated with imatinib. No recurrence or metastasis was found after a 6-month follow-up. We identified 14 cases of prostatic primary EGIST in PubMed and summarized these cases with our case. The patients’ ages ranged from 31 to 78 years (average: 53.6 years), and most patients’ prostate-specific antigen (PSA) concentrations were within normal limits (92.9%, 13/14). All patients underwent imaging examinations; prostatic masses measured 6 to 14.2 cm (mean: 9.43 cm), and imaging excluded secondary prostatic masses from the intestinal tract. By immunohistochemical staining, the tumors were positive for cluster of differentiation (CD)117 (71.4%, 10/14), DOG1 (100%, 7/7), and CD34 (100%, 14/14), and negative for smooth muscle actin (SMA) (71.4%, 10/14), desmin (100%, 11/11), and S100 (100%, 12/12). Treatment depended on the results of the gene mutation detection as well as the risk estimation according to tumor size and microscopic mitotic rates (>5 per 50 high-power fields: 60%, 6/10). Among the 12 patients with reported outcomes, nine achieved good results (no recurrence or metastasis), one achieved reduced mass volume, one experienced recurrence, and one died.
Introduction
Gastrointestinal stromal tumor (GIST) is the most common soft tissue sarcoma in the digestive tract. 1 In a small number of cases, mesenchymal tumors originate from outside the gastrointestinal tract, with histomorphology, immunohistochemical molecules, and gene mutation sites similar to those in GIST. These mesenchymal tumors are called extra-gastrointestinal stromal tumors (EGIST), and among them, prostatic EGISTs are, peculiarly, extremely rare. To our knowledge, only 14 cases of primary EGIST of the prostate have been reported in the English-language literature to date. In this study, we reported the details of a 62-year-old man with primary prostatic EGIST.
Case report
A 62-year-old man presented to the Department of Urology at Tongji Hospital affiliated to Tongji Medical College of Huazhong University of Science and Technology with progressing dysuria and urgency for 6 months. Trans-rectal prostatic ultrasonography indicated a markedly enlarged prostate, while digital rectal examination demonstrated an enlarged prostate with unusual consistency on palpation. The serum prostate-specific antigen (PSA) concentration was 1.2 µg/L, and the carcinoembryonic antigen (CEA) concentration, as well as other laboratory values, were within the normal ranges. Pelvic magnetic resonance imaging (MRI) revealed that the prostatic mass measured 9.5 × 4.8 × 9.5 cm3, presented as mixed hypointense T1 signals and hyperintense T2 signals, and compressed the bladder, seminal vesicle, and rectum.
There was no evidence of rectal infiltration (Figure 1a and b), and no enlarged pelvic lymph nodes were detected. Whole-body bone scan (multi-probe) and chest roentgenography identified no metastases, and abdominal plain computed tomography (CT) showed no abnormalities. Thus, a primary prostatic mass was preliminarily diagnosed. To further investigate the pathological nature of the mass, trans-rectal ultrasound-guided prostatic biopsy was subsequently performed, and post-operative pathology revealed that spindle-dominant tumor cells proliferated and showed mild cytological atypia. There were no typical areas of coagulative neoplastic necrosis, and low mitotic counts (<5 per 50 high-power fields) were observed (Figure 2a–c). Immunohistochemical stains for cluster of differentiation (CD)117, CD34, DOG1, smooth muscle actin (SMA), and H3K27Me3 were diffusely positive, and staining for desmin (DES), S100, anti-pan-cytokeratin antibody (PCK), caldesmon, and SOX10 was negative (Figure 3a–g). The imaging evidence and histological results indicated a diagnosis of primary prostatic EGIST. To obtain more information for treatment planning and to further confirm the EGIST diagnosis, gene mutation examination revealed missense mutation in ARID1A exon 3 and deletion mutation in c-kit exon 11, indicating expected prolonged survival benefit with imatinib therapy. The patient received targeted imatinib therapy (400 mg, daily) and was followed for 6 months. The tumor volume decreased to 1.5 × 0.8 × 1.3 cm3 (examined in a local hospital), and the patient experienced no metastasis or recurrence. For personal reasons, the patient refused radical prostatectomy.
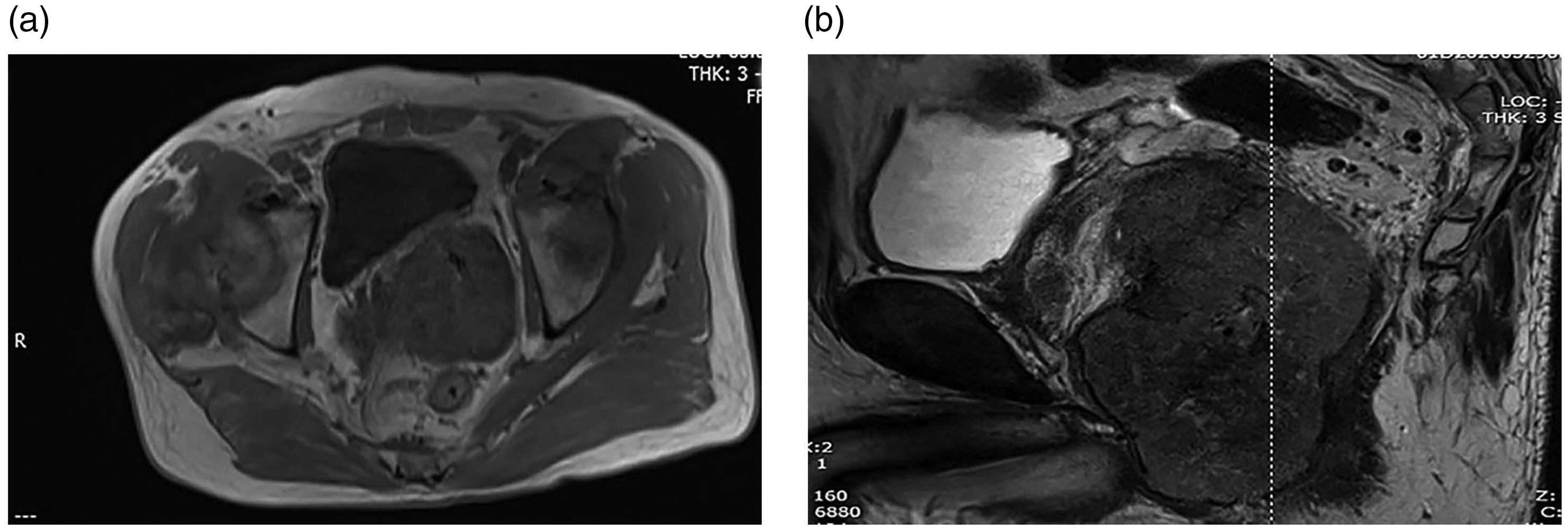
Magnetic resonance imaging showing a markedly enlarged prostate occupied by a heterogenous mass expanding and compressing the seminal vesicle. (a) coronal view; (b) sagittal view.

Microscopy (histology) of the biopsy specimen. The tumor cells are mainly spindle-shaped, with mitotic numbers < 5 per 50 high-power fields (HPF) and with no obvious tumor necrosis (magnification: a, ×10; b, ×20; c, ×40).

Immunohistochemical analysis of the tumor cells. The tumor cells stained diffusely and positively for cluster of differentiation (CD)117 (a), CD34 (b), DOG1 (c), and H3K27Me3 (d), and negatively for desmin (DES) (e), and S-100 (f). The Ki-67 index (g) was approximately 5 (all magnifications, ×40).
Discussion
GISTs account for approximately 4% to 7% of soft tissue sarcomas in the abdominal cavity; 2 EGIST is relatively rare. Since Van Der Aa et al. 3 reported the first case of primary prostatic EGIST in 2005, only 14 cases3–16 in the English language appear in PubMed. We performed a pooled analysis of these 14 patients, plus our case (Table 1). Among the 15 patients, except for missing PSA data for 1 patient, most of the PSA values were within the normal range (13/14 cases, 92.9%). Because PSA is secreted mainly by human prostatic epithelial cells, this result may support the suspicion that EGIST is a tumor composed of Cajal mesenchymal cells (interstitial cells of Cajal, ICC), their precursors, and other cells closely related to ICCs. 17 Most patients with primary EGIST first reported lower urinary tract symptoms, occasional anal region pain, perineal pain, and constipation. In addition, one asymptomatic case had a prostatic mass detected during routine physical examination. Imaging examination, mainly MRI and CT, is an important auxiliary means of diagnosing EGIST. Imaging can effectively measure the tumor size, judge the degree of adhesion with surrounding tissues, such as the rectum, and distinguish prostatic invasion, which is the key to the differential diagnosis of primary prostatic EGIST and secondary extended GIST from intestinal tract tumors. Other imaging methods, such as 18 F-fluorodeoxyglucose positron emission tomography (18F-FDG PET)/CT, can also contribute to diagnosis, staging, restaging, and monitoring the treatment response of EGIST. 6
Prostatic EGIST cases reported in PubMed.

PSA, prostate-specific antigen; TURP, transurethral prostatectomy; RP, radical prostatectomy; LOH, loss of heterozygosity; N/A, not available; CD, cluster of differentiation; SMA, smooth muscle actin; Vim, vimentin; CK, cytokeratin; RALP: robot-assisted laparoscopic prostatectomy; HPF: high-power field; PDGFRA, platelet-derived growth factor receptor-α; PCK, anti-pan-cytokeratin antibody.
The histomorphological features, immunohistochemical biomarkers, and molecular biological characteristics of EGIST are similar to those of GIST. The pathological features of GIST include fusiform and/or epithelioid, polymorphic cells; spindle cells (70%) are the most common cell type in EGIST tissues. Cells are spiral-shaped with clumped cytoplasm, pale red, unclear membranes, even staining, and unclear nuclei. Epithelioid cells (20%) are round cells arranged in a wheel-like and nest-like manner. The cytoplasm is pink and clear, the nuclei are eccentric, nucleoli are small, and the staining is uniform. Immunohistochemically, DOG1 (positivity rate: 92%) and CD117 (positivity rate: 81%) are the most sensitive and specific antibodies for diagnosing GIST. 18 Other molecular markers that can assist in diagnosis are CD34 and the very specific markers, SMA and desmin, as well as the neural marker, S100. For the 15 cases of primary prostatic EGIST, the positivity rates of each molecule were as follows: CD117 (71.4%, 10/14), DOG1 (100%, 7/7), and CD34 (100%, 14/14); the negativity rates were as follows: SMA (71.4%, 10/14), desmin (100%, 11/11), and S100 (100%, 12/12).
In 1998, Hirota et al.’s 19 pioneering study showed that gain-of-function mutations of c-kit are the driving events causing cancer in GIST. The c-kit and platelet-derived growth factor receptor-α (PDGFRA) mutation patterns in EGIST were similar to those in GIST; mutation of c-kit exon 9 or 11 was the most common type (accounting for approximately 70% of all mutations), and PDGFRA mutations were found in a smaller number (5%–10%) of exons 12 or 18. Detection of EGIST mutations can be used not only to diagnose EGIST but also to guide patients' subsequent treatment options. Since the development and proven efficacy of imatinib, a molecularly-targeted drug targeting mutations in GIST c-kit and PDGFRA genes, the median patients’ overall survival increased from 18 months to 5 years, 20 with a significant survival benefit. The response of imatinib was most prominent in patients with mutated c-kit exon 11, with 400 mg/day as the constant effective dose, while with mutated c-kit exon 8, a dose of 800 mg/day was usually required to achieve the optimal clinical response. Thus, patients with mutations at these sites usually have a better prognosis. Other prognostic factors associated with EGIST are age, sex, mitotic index, high ki-67 index (≥10%), tumor size, necrosis, and histological type.21–23 Lee et al. 24 also reported that negative c-kit expression was an independent prognostic indicator of overall survival. According to the National Cancer Institute (NCI) Consensus Meeting (Table 2, Demetri et al.), 25 EGIST can be graded for risk according to tumor size and microscopic mitotic index. Among the 15 patients with prostatic EGIST, 8 patients underwent genetic testing, and the c-kit exon 11 mutation rate was 87.5% (7/8). No PDGFRA mutation was found in these eight patients. The mean age of the 15 patients was 51.9 years (range, 31–78 years), the mean tumor size was 9.42 cm (range, 6–14.2 cm), 6/10 tumors (60.0%) had > five mitotic figures per 50 HPFs, and the mean follow-up period was 19.3 months (6–49 months). Except for one case of liver metastasis at admission, one case of recurrence at 49 months, and one death after 6 months due to intermittent non-prescribed medication, no cases (n = 9) showed recurrence or metastasis (data were unavailable for three cases).
Risks related to adverse outcomes, such as metastases (according to the NCI Consensus Meeting, Demetri et al. 25

HPF, high-power field.
There is currently no consensus regarding the treatment plan for EGIST; treatment plans are devised according to the patient’s risk classification. However, combining experience from EGIST diagnosed in other primary sites,27–30 with all prostatic EGIST cases included in this study, for prostatic EGIST, we propose radical prostatectomy (RP) for medium- and low-risk tumors; RP + adjuvant therapy or neoadjuvant therapy + RP + adjuvant therapy for medium- and high-risk tumors. Conservative treatment with imatinib alone appears to work well for patients who have lost the chance for surgery or who decline surgery. We emphasize that this treatment plan is based on limited evidence, and further studies are needed.
Limitations
Owing to the rarity of EGIST, extensive evaluations are difficult.
Conclusion
We reported a very rare case of primary prostatic EGIST, and we pooled and analyzed the characteristics of all 15 patients (including our case) reported to date. The majority of patients with prostatic EGIST are diagnosed with lower urinary tract symptoms, and patients usually have normal PSA concentrations. Prostate masses can be found by MRI or CT examination. Microscopically, the tumor tissues show similar histomorphological characteristics with those of GIST. In most tumors, CD117 and DOG1 are positive, and CD34 could be positive; SMA, desmin, and S100 are negative. Patients should be graded for risk according to tumor size and mitotic rates. Additionally, c-kit exon 11, PDGFRA exons 12 and 18, and other mutation-prone sites should be evaluated to guide subsequent treatment.
This report was written in accordance with the Equator CARE Guidelines. 26
Footnotes
Ethics statement
No ethical approval was required for case reports in China at the time of this study. However, we sought and obtained approval (No. TJ-C20210413) after the study (15 April 2020). The authors obtained written informed consent for treatment and publication from the patient.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
XZ provided the patient’s data; LL analyzed the data and was a main contributor in writing this manuscript; JHG, CJK, and JHT helped with data collection; CGY and ZQH provided guidance and advice. All authors have read and approved the manuscript.