
Abstract
A 57-year-old woman presented to her ophthalmologist because of rapid deterioration in vision. Dilated funduscopic examination of the right eye showed an elevated, yellow-orange choroidal mass temporal to the fovea; a complete retinal detachment was present in the left eye. The patient was referred to an oncologist. Computerized tomography of the brain, thorax, abdomen, and pelvis were obtained. They revealed an 11-mm mass in the right parietal lobe, a 30-mm mass in the left temporal lobe, 23-mm mass in the right kidney, and multiple nodules in both lungs. Supported by published experience with intravitreal bevacizumab for choroidal metastasis, the patient was injected into the vitreous through the pars plana of the left eye. The tumor mass did not show signs of regression and the visual acuity was unchanged. The patient suffered from end-state complications tumor metastasis and expired one month after the invitreal injection.
Case Report
A 57-year-old woman of Italian and Spanish parentage presented to her ophthalmologist in December 2009 because of rapid deterioration in vision. She had had headaches for the preceding six months. On examination, visual acuity was 20/200 OD and hand motions OS. Applanation tonometry was 12 mm Hg OD and 10 mm Hg OS. Dilated funduscopic examination of the right eye showed an elevated, yellow-orange choroidal mass temporal to the fovea (Figure 1A); on fluorescein angiography, late hyperfluorescence was present in the late arteriovenous phase. A complete retinal detachment was present in the left eye.
Fundus photographs and selected fluorescein angiograms of the right eye. A) Prior to injection of bevacizumab, an elevated yellow-orange choroidal mass in the temporal posterior pole is noted (asterisk); B) fluorescein angiogram shows leakage associated with the choroidal mass (asterisk); C) the mass is unchanged twelve days after bevacizumab treatment (asterisk); D) hyperfluorescence (pooling) on fluorescein angiogram twelve days after treatment (asterisk).
The patient was referred to an oncologist. Computerized tomography of the brain, thorax, abdomen, and pelvis were obtained. They revealed an 11-mm mass in the right parietal lobe, a 30-mm mass in the left temporal lobe, 23-mm mass in the right kidney (Figure 2A), and multiple nodules in both lungs (Figure 2B). Computerized tomogram of the pelvis was normal. The renal mass and acute vision loss led to the suspicion that the choroidal lesion was a metastasis. Therefore, the oncologist recommended biopsy of the right kidney mass for pathologic diagnosis. Supported by published experience with intravitreal bevacizumab for choroidal metastasis, 1 bevacizumab (Avastin; Genentech, Inc, South San Francisco, California), 1.25 mg/0.05 mL, was injected via a 25-gauge needle into the vitreous through the pars plana of the left eye using a standard sterile protocol; topical moxifloxacin 0.5% drops (Vigamox, Alcon, Fort Worth, TX) were prescribed for five days. Five days after the injection, the visual acuity was unchanged; twelve days later, visual acuity was count-fingers. The tumor mass did not show signs of regression (Figure 1C). Fluorescein angiography continued to demonstrate hyperfluores-cence (Figure 1D). Based on results of sonography, computed tomography and magnetic resonance imaging, and so as to avoid complications of systemic chemotherapy, her doctors decided to initiate radiation therapy to the kidney alone. Twenty days after the intravitreal injection, the visual acuity was hand motions. Dilated funduscopic examination revealed an inferior retinal detachment; the choroidal mass was unchanged. The following day, the patient developed a total retinal detachment. Biopsy of the right kidney mass indicated that the primary tumor was (occult) ovarian serous cystadenocarcinoma (Figure 3). The patient suffered from end-state complications tumor metastasis and expired one month after the invitreal injection.
Computed tomographic (CT) scans of abdomen and thorax. A) unenhanced CT scan of the abdomen shows a mass lesion in the kidney; B) unenhanced CT scan of the thorax shows lesions in the lungs and mediastinum.
Biopsy of renal metastasis. A) Cell are pleiomorphic and hyperchromatic. They have high nuclear-cytoplasmic ratio and numerous mitoses (hematoxylin and eosin stain). B) Tissue stains for cytokeratin 7, a basic cytokeratin found in many glandular and transitional epithelia and their neoplasms.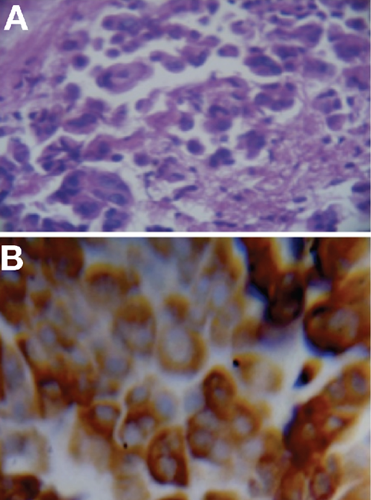
Discussion
This report describes a patient whose choroidal metastasis from occult ovarian serous cystoadenocarcinoma did not respond to intravitreal bevacizumab. This case stands in contrast to a case we described of a patient whose choroidal metastasis from colon carcinoma resolved and whose visual acuity improved markedly after intravitreal bevacizumab. 1 Reasons for failure in other cases may be that ovarian tumors and their metastases are not solely dependent on vascular endothelial growth factor (VEGF) for their survival as may be the case in colon cancer, that VEGF is sequestered in the extracellular matrix components of ovarian tumors and therefore not biologically relevant, or that VEGF expression in metastases may be heterogeneous. When evaluated in combination with chemotherapy, bevacizumab was associated with improved long-term outcomes in other tumors, leading to approval by the United States Food and Drug Administration (FDA) for use in metastatic colorectal cancer, non-squamous non-small cell lung cancer, glioblastoma multiforme, metastatic renal cell cancer, and recurrent breast cancer (the approval for which the Food and Drug Administration revoked in December 2011). Bevacizumab is not approved for ovarian cancer; studies are ongoing as to its role in targeted therapy for ovarian cancer and optimizing chemotherapy for ovarian cancer.2,3 Ovarian serous cystadenocarcinoma accounts for 90% of all ovarian carcinomas. Malignant epithelial ovarian cystadenocarcinomas are the only ovarian cysts associated with racial differences; women from northern and western Europe (like our patient) and North America are affected most frequently, whereas women from Asia, Africa, and Latin America are affected least frequently. 4 The molecular mechanisms that govern ovarian cancer metastasis must be understood in order to treat this disease.5–10 Multiple adhesion molecules, cytokines, growth factors and extracellular matrix components are involved in ovarian cancer cell differentiation state and metastatic potential.8–10 Since high-grade serous ovarian cancer is characterized by over-expression of VEGF, interception of this pathway can be achieved through engineered binding site molecules or through monoclonal antibodies to VEGF, the most widely studied agent being bevacizumab. 11
However, data from studies of bevacizumab as concurrent therapy followed by maintenance therapy with bevacizumab or placebo for serous ovarian carcinoma suggest that VEGF blockade may have greater impact in preventing tumor regrowth, or in the management of recurrent disease, rather than augmentation of primary chemotherapy. 12 One reason may be that ovarian tumors are avascular tumors that derive sufficient oxygen and nutrients by simple passive diffusion. 13 To help explain the variable effect of intravitreal bevacizumab in different choroidal metastases, perhaps VEGF expression in metastases is heterogeneous among multiple metas-tases. 13 Yet another possible reason for failure of bevacizumab to induce regression is that VEGF in a tumor may be sequestered in extracellular matrix components. VEGF can bind to a number of other circulating proteins, not just to VEGF receptors, but presumably, only the VEGF-receptor compound is biologically relevant. 13 This notion is supported by pharmacokinetic findings regarding the spatial distribution of VEGF iso-forms and their interactions with heparan sulfate in the extracellular matrix and metalloproteinases which cleave and induce the VEGF-mediated tumorigenesis.14–20 In individual case reports, intravitreal bevacizumab has been described as leading to the regression of choroidal melanoma,21,22 regression of iris metastasis from small-cell lung cancer, 23 and regression of symptomatic circumscribed choroidal hemangioma with subretinal fluid. 24 To our knowledge, there has been no report of the effect of intravitreal injection of bevacizumab on a choroidal metastasis from ovarian carcinoma. In recent years with a better understanding of the role of angiogenesis, many cancer therapies have targeted specific mechanisms of tumor growth and metastasis. However, it is challenging to predict the effects of VEGF-neutralizing agents,25–28 since angiogenic tumors can adapt to the presence of neovascularization inhibitors by acquiring the means to evade the blockade of angiogenesis pathways.29,30 Both tumor progression and mortality may follow a period of therapeutic response, while the tumor develops an adaptive response that mediates tissue matrix invasion.31–33 In contrast, patients like the one described here, in whom there seems to be no therapeutic response at all, may have tumors possessing an intrinsic resistance to angiogenesis inhibitors.
Conclusions
In conclusion, intravitreal bevacizumab had no effect on the choroidal lesion or on recovery of visual acuity in this case of choroidal metastastasis from ovarian carcinoma. It is possible that the effect of bevacizumab on a choroidal metastasis is correlated with its effect on the primary tumor (bevacizumab not being the first-line treatment for ovarian carcinoma) or that expression of VEGF is heterogeneous or sequestered so as not to be biologically relevant. Longer follow up is required in cases where intravitreal bevacizumab has been reported to lead to regression of choroidal metastasis. These results may help guide practitioners as to which cases to choose intravitreal bevazimab injections.
Footnotes
Acknowledgements:
The authors would thank Dr. Ruben Sambuelli for immunohistochemical studies.