
Abstract
Testicular fibroma of gonadal stromal origin is a rare benign tumor of testis which usually presents as a slow growing testicular mass. Only 25 cases of testicular fibroma have been reported in the literature. Presence of minor sex cord elements in this tumor is even rarer. We report a case of testicular fibroma with minor sex cord elements that involved almost the entire testis and tunica vaginalis. The patient presented with hydrocele, a rare presentation for this entity. The rarity of the diagnosis and the clinical presentation prompted this case report.
Introduction
Benign intrascrotal fibrous lesions are rare, with most arising in the paratesticular region. Intratesticular fibrous tumors are even more uncommon. 1 In previously published reports they were described under different names such as diffuse stromal form of gonadal stromal tumor, 2 thecoma like sertoli cell tumor, 3 testicular fibroma, 4 theca cell tumor, 5 myoid gonadal stromal tumor with epithelioid differentiation, 6 to name but a few. According to the recent WHO classification they are considered as sex cord/gonadal stromal tumors and classified under the tumors of thecoma/fibroma group. 7 Testicular fibromas are analogous to similar tumors in the ovary. We report a case of testicular fibroma containing minor sex cord elements. To date only 25 cases of testicular fibroma have been reported and presence of minor sex cord elements in this tumor is even rarer. 8
Case Report
A 40-year old male presented with painless scrotal swelling that had gradually increased in size for two years. He had no hormonal symptoms. On examination, enlarged firm left testis and hydrocele with positive translucency test was detected. The ultrasonogram (Figure 1A) showed grossly enlarged left testis measuring 7.6×4.5 cm with diffusely heterogeneous echo-texture. There were multiple well-defined nodular and heterogeneously echoic lesions found within the left scrotum adherent to the wall. A large amount of free fluid was seen in the left scrotal sac. The right testis and epididymis were unremarkable. The patient had undergone testicular FNAC one year before and mesenchymal tumor had been diagnosed. A review of slides revealed cellular smear with 3-dimensional clusters and groups composed of bland looking spindle cells (Figure 1B).

A) Ultrasonography showing testicular SOL with diffusely heterogeneous echo-texture and fluid in the scrotal sac; B) cellular smear showing cluster of bland spindle cells (May-Grunwald-Giemsa, ×400); C) cut section of enlarged testis showing grey-white, mostly solid and a few cystic areas. Tunical sac is partially attached to the testis; D) tunical sac is showing multiple well circumscribed nodules of varying sizes. Thin rim of normal appearing testicular tissue is present.
The patient underwent left high inguinal orchidectomy and the specimen was sent for histopathological examination. The testis was firm, measuring 7.5×7×6.5 cm, and had a partially attached tunical sac which contained multiple well-defined nodules on its inner surface. The cut surface of the testis was gray-white, mostly solid, with few cystic areas (Figure 1C). A thin rim of normal appearing testicular tissue was present (Figure 1D). Microscopically, sections from the testis and the tunical sac nodules showed nests of spindle cells arranged in bundles separated by variable amounts of collagen (Figure 2A). The nuclei were fairly uniform with evenly dispersed chromatin and mitotic figures of up to 2 MF/10 high power fields were present. Occasional foci showed tubules which were lined by cuboidal cells and contained central hyaline materials (Figure 2B). On immunohistochemical examination, the tumor cells showed strong immunoreactivity for vimentin (Figure 3A) and were immunonegative for calretinin, WT-1, inhibin, pancytokeratin, cytokeratin 5/6, smooth muscle actin, CD 34 and S 100 protein. The ki 67 proliferative index was 2% (Figure 3B). Lining cells of the tubule were immunoreactive for inhibin (Figure 3C). The post-operative period was uneventful and there was no evidence of disease after a follow-up period of six months.
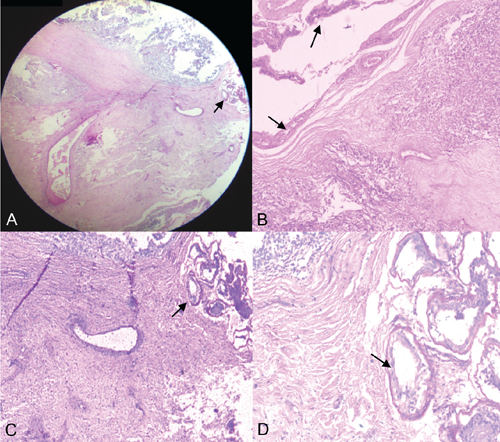
Sections show bundles of bland spindle shaped cells separated by fibrocollagenous stroma and a few tubules (arrow). A) Haematoxylin and Eosin, ×40; B) Haematoxylin and Eosin, ×100; C) Periodic Acid Schiff, ×100; D) Periodic Acid Schiff, ×400.

A) and B) cluster of tubules which are lined by inhibin positive cuboidal cells (×100 and ×400 respectively). B) Spindle cells showing diffuse strong cytoplasmic positivity for vimentin (×200). D) The Ki-67 proliferative index was 2% (×400).
Discussion
According to the recent WHO classification, testicular fibromas of gonadal stromal origin are classified under the sex cord/gonadal stromal tumor. Testicular fibromas are reported in men with an average age of 39±4.2 years (range 16-67 years). 1 The tumor presents as a slow-growing, sometimes painful mass that is not associated with hormonal alteration. Neither recurrence nor metastases have been observed. Testicular tumor markers, α-fetoprotein and β-human chorionic gonadotropin levels are normal. Our case presented with hydrocele which is an unusual presentation for this tumor.
These tumors are firm, well circumscribed, rarely encapsulated nodules, measuring 0.8-7 cm in diameter. 8 They are yellow-white to white in color, without hemorrhage or necrosis. In our case, almost the entire testis was replaced by the tumor, measuring 7.5 cm at its widest diameter, with simultaneous nodules on the inner surface of tunica vaginalis. These macroscopic features are unusual for testicular fibroma. Microscopically, intratesticular fibromas are composed of short, randomly interweaving fascicles of spindle cells displaying a storiform pattern separated by fibrocollagenous stroma that may be hyalinized. Mitotic activity generally ranges from 1 to 2 per 10 high-power fields, but can reach up to 4 per 10 high-power field. 9 Our case had similar microscopic features with a few foci of solid tubules lined by inhibin positive cuboidal cells representing minor sex cord elements. A similar minor sex cord component of less than 10% of tumor has been described in some cases of ovarian fibroma. There have been few reported cases of testicular fibroma with minor sex cord elements in the literature. On immunohistochemistry, testicular fibromas are positive for vimentin,6,9–13 smooth muscle actin,6,9,12 and, occasionally, are reactive for desmin, 9 cytokeratin, 13 or S-100 protein.10,12 Inhibin and CD 99 are non-reactive. In this case, only vimentin immunostain was positive. Differential diagnosis includes rare cases of intratesticular leiomyoma, intraparenchymatous growth of neurofibroma, solitary fibrous tumor and sarcomatoid mesothelioma of tunica vaginalis. 9 Testicular leiomyoma are positive for a-smooth muscle actin, desmin and h-caldesmon. Testicular fibroma can also be reactive for smooth muscle actin, though not in our case. Presence of minor sex cord component in testicular fibroma helps differentiate between these two tumors. Neurofibroma is immunoreactive for S-100 protein but negative for smooth muscle actin, desmin and inhibin. Solitary fibrous tumor of tunica vaginalis is CD 34 positive. Sarcomatoid mesothelioma is usually immunoreactive for cytokeratin (AE1/AE3), calretinin and vimentin, and variably positive for WT-1, podoplanin, smooth muscle actin and cytokeratin 5/6. The combination of a broad spectrum cytokeratin with calretinin combines both high sensitivity (77% for AE1/AE3) with high specificity (100% for calretinin) for sarcomatoid mesothelioma and can be diagnostically useful. 14
Conclusions
Testicular fibroma of gonadal stromal origin with or without minor sex cord elements is considered a benign neoplasm. Knowledge of this rare tumor is important as it can be successfully treated by conservative surgery.
Footnotes
Acknowledgments
The authors appreciate the support received from the technical staff of the Department of Pathology, Nilratan Sircar Medical College, Kolkata and Dr. Sanjay Navani, Lab Surgpath, Mumbai for help in immunohistochemistry.