
Abstract
Primary bone tumors can be either benign or malignant considering their natural history and cellular morphology. Benign bone tumors are much more frequent than malignant ones although some of them like giant cell tumor of bone can behave just like a malignant one that means has the capacity for massive local destruction and remote metastasis. Giant cell tumor of bone in adult people has a very strong and diagnostic predilection for epiphysial location in long bones. Very few cases have been so far reported for a giant cell tumor of bone with non-epiphysial location in a long bone.
Introduction
Giant cell tumor of bone is a primary benign bone neoplasm that includes 5% of all bone neoplasms.1,2 They typically occur in patients between the age of 20 and 40 years and there is a slight female predominance.1–3 Giant cell tumor of bone usually are solitary, however, 1% to 2% may be multicentric. 4 The natural history of this lesion has been studied widely before and it has been well noticed that this tumor has a strong predilection for epiphysis of long bones after closure of growth plate. In spine, the sacrococcygeal area and upper cervical spine is a common site for occurrence of this tumor. 5 Although metaphyseal location is commonly encountered in young adults before closure of growth plate, this has been reported in only 2% of adult people. 6 In the study performed in Mayo Clinic on 567 patients suffering from giant cell tumor of bone, they found just 6 patients with metaphysial location from them only 2 were above 20 years of age. 7 No patient in that study had diaphyseal or even meta-diaphyseal lesions.
Mirra et al. observed that without an underlining disease such as Hyperparathyroidism no giant cell tumor can extend beyond epiphysis in adults.
We are introducing an adult female patient that was referred to our clinic because of a destructive lesion of her left femur in the meta-diaphyseal location. Because of her age and pattern of the lesion she underwent an open incisional biopsy that the result was compatible with primary bone giant cell tumor. There was no other associated disease justifying the diagnosis.
Case Report
A 46 years old otherwise healthy female patient was referred to our clinic because of a bone lesion in her left femur. She noticed deep aching pain in her left thigh two months earlier. She denied any history of trauma or any febrile episode during that period. The patient was seen by different physicians and finally an orthopedic surgeon did order a plain X-ray that showed a destructive bone lesion in her left distal femur with a permeative pattern (Figure 1). Computed tomography (CT) scanning (Figure 2) and magnetic resonance imaging (MRI) (Figure 3) showed that the lesion was located in meta-diaphysial area and it had eroded the anterior bone cortex of left femur, but there was no soft tissue extension by the lesion.

X-ray show a destructive bone lesion in the left distal femur.

Computed tomography scan shows the lesion, located in meta-diaphysial area.

Magnetic resonance imaging showed that the lesion was located in meta-diaphysial area and it had eroded the anterior bone cortex of left femur.
All laboratory data including CBC, blood calcium, Phosphorus and Alkaline-Phosphatse level was within normal limits. Serum parathyroid assay reported to be within normal range. All other staging studies including chest and abdomen CT scan and whole body bone scanning was negative for any other abnormal lesion. Because of her age and the pattern of the lesion, she underwent an open incisional bone biopsy. The result was compatible with primary giant cell tumor of bone (Figure 4).
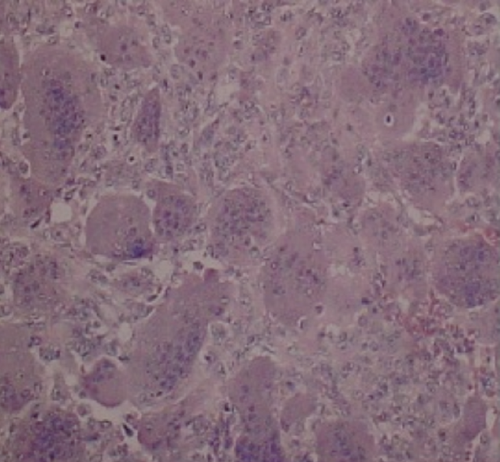
Primary giant cell tumor of bone (Haematoxylin and Eosin).
Subsequently she underwent curettage and internal fixation with a side plate augmented with bone cement. She did recover uneventfully and so far with a follow-up of 24 months she is doing good and there is no local recurrence for the lesion detected.
Discussion and Conclusions
Giant cell tumor of bone is a common primary benign bone lesion with unknown origin. 8 According to Enneking's staging system it often presents as an active stage two lesions although transition to aggressive stage three is not unusual. 9 The tumor has a strong predilection for epiphysial location although in young ages before closure of growth plate this tumor can happen in metaphysis of long bones. Diaphysial location in adults rarely if ever been reported. Here we are presenting an adult female patient with a meta-diaphysial lesion of femur that the incisional biopsy confirmed the diagnosis of benign giant cell tumor of bone. All other laboratory and staging studies failed to show any other disease or hormonal imbalances. Patient underwent definitive surgery with wide curettage and internal fixation augmented with bone cement and there encountered no local recurrences in two year follow-up. 10