
Abstract
A 57-year old man was referred to the Urology Department due to gross hematuria; abdominal ultrasound revealed an unspecific solid tumor of the left bladder wall. Ultrasound, transurethral resection of the bladder mass with subsequent histological analysis, thoracic and abdominal computed tomography-scan and brain magnetic resonance imaging were performed. He was diagnosed with a bladder metastasis of clear cell renal cell carcinoma (RCC) with concomitant bone, pulmonary, and cerebral metastatic disease of a primary RCC of the right kidney. Management: Transurethral resection of the bladder mass, cerebral and bone radiotherapy, removal of the primary tumor, targeted systemic therapy with mTOR followed by tyrosine kinase inhibition.
Introduction
Renal cell carcinoma (RCC) is the most common kidney tumor. Approximately 64,770 new cases of kidney cancer are diagnosed each year. In 2012, this resulted in approximately 14,000 deaths in the United States with a growing trend. 1 Approximately one third of RCC patients has metastatic disease at the initial diagnosis and 30% of all patients will develop distant metastases later on. 2 The lung (75%), liver (40%), bone (40%), soft tissues (34%) and pleura (31%) are the most frequent sites of RCC metastasis. 3 In accordance, metastatic RCC is also seen as a clinical chameleon due to its ability to metastasize almost to any organ within the body, including the thyroid, pancreas, spleen, skin, intestine, heart, but also the urinary bladder. 4 Interestingly, metastatic disease in these organs often occurs as metachronous metastasis, even years after the initial diagnosis. However, the metastatic spread from RCC to the urinary tract especially to the bladder is a rare event and is described in less than 2% of patients with less than 30 cases published in literature.5–7 Here, we report the case of a male patient with asymptomatic gross hematuria, diagnosed with a solitary, synchronous bladder metastasis of an advanced RCC of the right kidney with concomitant bone, pulmonary, lymphatic and cerebral metastatic disease.
Case Report
A 57-year-old man was referred to the Department of Urology due to painless and recurrent gross hematuria. Urine analysis revealed no signs of urinary tract infection. Ultrasound revealed a solid and undefined bladder mass located at the left bladder wall in close position to the bladder neck and in addition a tumor in the right kidney was found (Figure 1). At initial presentation, the patient reported a good quality of life and had an Eastern Cooperative Oncology Group performance status (ECOG=0) without further symptoms. The patient underwent an initial thoracic and abdominal computed tomography (CT) scan which confirmed the renal tumor of the lower kidney pole (4.3x4.2x4 cm, Figure 2A, B) with the suspicion of hilar lymph node metastasis and the suspicious bladder lesion (2.1x1.9x1.8 cm, Figure 2C, D). In addition the CT scan exposed multiple bilateral pulmonary metastases, enlarged mediastinal lymph nodes, instable bone lesions of the lumbar spine and the left femur. Due to the new onset of severe headaches a cerebral examination by magnetic resonance imaging was done three weeks later and showed four cerebral metastases in both hemispheres with no further sensorymotor neurological symptoms to be present. An initial transurethral resection of the bladder (TURBT) was performed to control gross hematuria and to retrieve histological tissue for the differentiation between urothelial and renal cell carcinoma. The pathologic examination demonstrated a metastatic RCC lesion located within the detrusor muscle of the bladder wall, which did not reach into the lamina propria mucosa (Figure 3). After TURBT a whole brain radiation with concomitant glucocorticoid medication and lumbar spine radiation was performed. In addition, the patients received zoledronic acid (4 mg once per month) for bone protection with the intention to reduce the risk of secondary bone events. At the end of the radiation the patient was again referred to the Department of Urology for the removal of the primary tumor in the right kidney; now the patients had an ECOG performance status of 1. Lumbar retroperitoneal radical nephrectomy with hilar lymphadenectomy was performed and final pathologic classification reported a pT1b, pN0, cM1 RCC, Fuhrman Grading 3. 8 The patient was discharged on the 10th postoperative day. Primarily planned systemic therapy of sunitinib malate was changed to mTOR inhibition by temsirolimus (25 mg i.v. weekly) due to a reduced postoperative ECOG score of 3 and poor risk categorization according to the Memorial Sloan-Kettering Cancer Center (MSKCC) criteria.9,10 Temsirolismus administration was initiated three weeks post surgery and was well tolerated without any sideeffects. The restaging showed a progressive pulmonal and bone metastatic disease without recurrence of the bladder lesion ten weeks after the start of systemic therapy. Due to lack of evidence-based second line treatment after mTOR based therapy failure, the therapy was switched to sunitinib malate 50 mg daily on a 4-weeks-on/2-weeks-off schedule. 11 The patient presented in reduced general conditions with ascites, general anasarca and symptoms of a paralytic ileus 6 weeks after the start of sunitinib malate. Systemic treatment was stopped and received palliative home care until his death two weeks later.

Ultrasonography of the bladder and the kidney: ultrasound examination reveals a suspicious bladder lesion at the left bladder wall (1.75× 1.98 cm, A) and a kidney tumor of the lower pole (5.24× 2.7 cm, B).
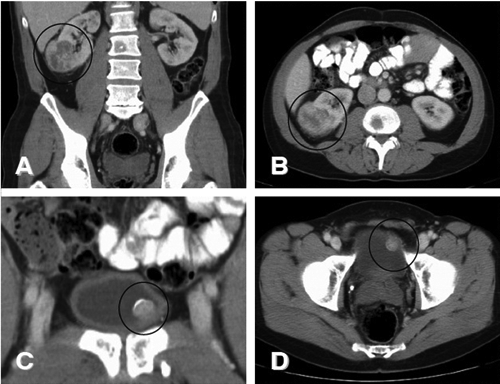
Abdominal computed tomogrphy scan demonstrates a right-sided renal tumor [coronar (A) and axial (B) reconstruction] and a left-sided bladder mass [coronar (C) and axial (D) reconstruction].
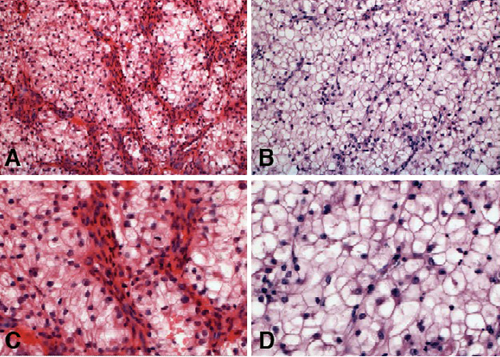
Bladder metastasis of a clear cell renal cell carcinoma: the histological examination showed a metastatic lesion located within the detrusor muscle of the bladder wall, which did not reached into the lamina propria.
Discussion
The classic Virchow s triad of hematuria, flank pain and palpable abdominal tumor occurs in advanced stage RCC in about 6-10% of patients. In this context, hematuria is principally considered as a symptom which indicates a renal pelvis infiltration and which can be regarded as a first sign of urinary tract involvement. 12 However, in the presented case, the initial symptom of gross hematuria led to the diagnosis of a synchronous RCC metastasis of the bladder. In addition, to the metastatic involvement of the bladder, the primary RCC lesion in the right kidney had already metastasized to the bone, lung and the brain.
Metastasis to the urinary tract is a rare event. It seems to be associated with an advanced tumor stage and a poor patient s prognosis with a reduced overall survival as described by several reports.13,14 Most of these reports describe a metachronous interval even of years after the initial diagnosis, before bladder metastases become apparent. Although synchronous bladder metastases are less frequently diagnosed, several case studies reported the synchronous spread of metastatic RCC.5–7 Nevertheless, the pathologic mechanism of urinary bladder involvement remains unknown. The lymphatic, hematogenous or transureteral tumor spread into the bladder is hypothesized. In this case the intramuscular localization of the tumor cells within the bladder detrusor without contact to the urothelial layer of the lamina propria mucosa suggests a hematogenous spread as the reason. In contrast, urinary spread can be suspected if the primary tumor invades into the renal pelvis or at least into the collecting duct. 15 Although, TURBT is mainly performed for diagnostic purposes one has to consider the importance of a complete surgical resection of metastasis in RCC management. In concordance, in this case no bladder recurrence occurred after the complete removal of the bladder mass, whereas unresected tumor lesions in this patient exhibited a generalized rapid progression. Consequently, TURBT can be regarded as an effective surgical treatment in RCC patients not only to control gross hematuria, but also local tumor growth which is in line with other bladder metastasis arising from different cancer entities.16–18
Conclusions
RCC metastases within the genitourinary tract are extremely rare. Therefore, a gross hematuria in RCC patients is generally seen as an indicator of a renal pelvis infiltration and not as the sign of metastatic spread to the lower urinary tract. Nevertheless, the urologist and oncologist should be aware of these rare events to prevent a preterm diagnosis, to distinguish an urothelial carcinoma of the bladder and to insure a complete resection of the bladder metastasis by TURBT.
Footnotes
Conflict of interests: AS, JB and SK received honorary from Pfizer.