
Abstract
Objectives
To compare two intrathecal anaesthetics, bupivacaine and levobupivacaine, for their effects on motor and sensory blockade and haemodynamics in patients aged ≥65 years undergoing transurethral resection of the prostate (TUR-P) or transurethral resection of the urinary bladder (TUR-M).
Methods
Patients scheduled to undergo TUR-P or TUR-M were randomized to receive either 3 ml (15 mg) 0.5% isobaric levobupivacaine (group L) or 3 ml (15 mg) of 0.5% hyperbaric bupivacaine (group B) for spinal anaesthesia. The onset time, maximum level and time to reach the maximum level of sensory and motor blockade were recorded. Changes to haemodynamic parameters were also recorded.
Results
The study randomized 100 patients: 57 to group L and 43 to group B. Levobupivacaine did not cause any significant changes in haemodynamic parameters, including systolic blood pressure, and showed a similar sensory block onset time compared with bupivacaine, but it had a significantly longer motor block onset time compared with bupivacaine.
Conclusion
These current findings suggest that levobupivacaine can be used as a substitute for bupivacaine for spinal anaesthesia in elderly patients ≥65 years of age undergoing elective TUR-P or TUR-M operations.
Introduction
There has been a significant increase in the mean survival age of the global population due to major advancements in medicine over the last century, which has resulted in a change in the age distribution curve because of the addition of elderly to the global population. There has been an escalation in the proportion of the population that is considered to be in old age (or as elderly people), defined as being ≥65 years: a rise from 4% of the total population in 1900 to 13% in 2010. 1
Although spinal anaesthesia provides some advantages for elderly people compared with general anaesthesia, it may still have some critical disadvantages. For example, early mobilization during the postoperative period, a minimal number of respiratory complications, continuity of analgesia and short hospitalization time are among the advantages of spinal anaesthesia compared with general anaesthesia, but hypotension and bradycardia are the two major disadvantages associated with spinal anaesthesia.2–6
Spinal anaesthesia is frequently used during urological operations because it provides some major advantages over general anaesthesia, such as a shorter time to onset of motor block, and it allows for the use of lower volumes of local anaesthetic.6,7 Although there is a degree of hypotension risk associated with spinal anaesthesia, it enables early detection of excessive fluid load and hyponatraemia. 3 Effective spinal anaesthesia is possible with the correct choice of local anaesthetic. Suitable local anaesthetics should provide effective anaesthesia and analgesia during the operation and should have no side effects. Levobupivacaine is a local anaesthetic that is relatively new to clinical practice.8–10 Levobupivacaine is an S(−) enantiomer of bupivacaine and both agents have similar pharmacokinetic properties.8–10 There are several studies that have reported that the cardiovascular and central nervous system-related side effects of levobupivacaine are less frequent than those experienced with bupivacaine.8–10 Some toxic effects can be seen with high doses of bupivacaine and when it is used for a long duration.8–10 Based on these reports,8–10 levobupivacaine is recommended as an alternative to bupivacaine for patients who experience cardiovascular system-related side effects. However, it has been emphasized that more studies must be conducted to investigate the effects of levobupivacaine in detail.8–10 Despite the fact that levobupivacaine has been widely used for obstetric and nonobstetric epidural anaesthesia, 8 there is still a lack of comparative clinical studies that focus on intrathecal levobupivacaine administration.
This study aimed to compare these two intrathecal anaesthetics, bupivacaine and levobupivacaine, for their effects on motor and sensory blockade and haemodynamics in patients aged ≥65 years who underwent spinal anaesthesia during transurethral resection of the prostate (TUR-P) or transurethral resection of the urinary bladder (TUR-M) operations.
Patients and methods
Patients
This randomized study enrolled patients who underwent TUR-P or TUR-M operations under spinal anaesthesia between January 2006 and March 2008 in the Department of Anaesthesiology and Reanimation, Faculty of Medicine, Akdeniz University, Antalya, Turkey. Patients aged ≥65 years with American Society of Anesthesiologists physical status 2–3 were included in the study. 11 Patients who were allergic to local anaesthetic agents were excluded from the study.
The study was approved by the Akdeniz University Ethics Committee of the Faculty of Medicine (12.12.2006; no. Ethics-497). Written consent was obtained from each patient to receive anaesthesia and verbal consent was obtained from each patient before anaesthesia was administered.
Anaesthesia and surgical procedures
All patients were closely monitored throughout the procedure. The monitoring included electrocardiography, noninvasive blood pressure monitoring and peripheral oxygen saturation measurements. Using a sealed envelope technique, the patients were randomly allocated to receive either bupivacaine (Marcaine® Spinal 0.5% Heavy; AstraZeneca, London, UK) or levobupivacaine (Chirocaine®, 0.5%; Abbott Laboratories, Abbott Park, IL, USA) for spinal anaesthesia. A 25 G spinal needle (Spinocan®; B Braun, Melsungen, Germany) was inserted, and after clear cerebrospinal fluid became visible, one of these two solutions was injected into the subarachnoid interspace: 3 ml (15mg) 0.5% hyperbaric bupivacaine or 3 ml (15 mg) 0.5% isobaric levobupivacaine. In order to reduce the risk of hypotension, intravenous prehydration was applied using 500 ml 0.9% NaCl given over 10–15 min to all of the patients who were administered either levobupivacaine or bupivacaine. Following prehydration, saline infusion (0.9% NaCl at 4 ml/kg per h) was continued until the end of the operation.
The TUR-P and TUR-M procedures were undertaken to allow the resection of prostate or bladder lesions and they were carried out in the lithotomy position. The anaesthetist (D.G.) was blinded to the drugs used for spinal anaesthesia.
Clinical assessments
Scoring system for recording the extent of sensory blockade based on the sensory dermatomes.
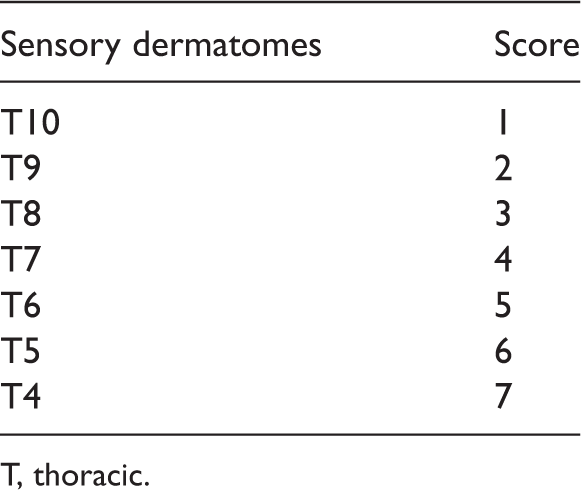
T, thoracic.
Systolic blood pressure (SBP), diastolic blood pressure (DBP), mean blood pressure (MBP), heart rate and peripheral oxygen saturation were measured before the operation, immediately after the intrathecal anaesthetic injection, at 5, 10, 15, 20, 25, 30, 45 and 60 min after the intrathecal anaesthetic injection and immediately after the operation was completed.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 11.0 (SPSS Inc., Chicago, IL, USA) for Windows®. The sample size was calculated for the power of this study being 50% (effect size was based on a pilot study of four patients in whom changes in heart rate and blood pressure after drug administration were observed). The two groups were compared using Student’s t-test when there was normal distribution of the data and Mann–Whitney U-test was used for the rest of the variables. χ2-test was used to compare categorical variables. Paired t-test was used for intergroup comparisons and for variables complying with normal distribution. Wilcoxon’s test was used for the rest of the variables. A P-value <0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of patients aged over 65 years who underwent spinal anaesthesia during transurethral resection of the prostate (TUR-P) or transurethral resection of the urinary bladder (TUR-M) operations, who were enrolled in a study to compare two intrathecal anaesthetics, 0.5% levobupivacaine (group L) and 0.5% bupivacaine (group B).

Data presented as mean + SD or number of patients (%).
Student’s t-test.
χ2-test.
No statistically significant between-group differences (P ≥ 0.05).
Sensory block data for patients aged over 65 years who underwent spinal anaesthesia during transurethral resection of the prostate (TUR-P) or transurethral resection of the urinary bladder (TUR-M) operations, who were enrolled in a study to compare two intrathecal anaesthetics, 0.5% levobupivacaine (group L) and 0.5% bupivacaine (group B).

Data presented as mean + SD.
P < 0.05 group L compared with group B; Student’s t-test.
NS, no statistically significant between-group difference (P ≥ 0.05).
Motor block data for patients aged over 65 years who underwent spinal anaesthesia during transurethral resection of the prostate (TUR-P) or transurethral resection of the urinary bladder (TUR-M) operations, who were enrolled in a study to compare two intrathecal anaesthetics, 0.5% levobupivacaine (group L) and 0.5% bupivacaine (group B).

Data presented as mean + SD.
P < 0.05 group L compared with group B; Student’s t-test.
NS, no statistically significant between-group difference (P ≥ 0.05).
In group L (levobupivacaine), the motor block score at 5 min after the intrathecal anaesthetic injection was significantly lower than the motor block score at 10 min and 15 min and the motor block score taken immediately after the operation was completed (P < 0.05 for all comparisons). The motor block scores at 20, 25, 30 and 45 min were similar to the motor block score taken immediately after the operation was completed and there were no significant differences between any of these time-points.
In group B (bupivacaine), starting from 10 min, the motor block score remained similar throughout the measurements and there were no statistically significant differences between subsequent time-points. The motor block score measured at 5 min after the intrathecal anaesthetic injection was relatively low and it was significantly lower compared with the scores recorded at all time-points and the motor block score taken immediately after the operation was completed (P < 0.05 for all comparisons).
Systolic blood pressure data for patients aged over 65 years who underwent spinal anaesthesia during transurethral resection of the prostate (TUR-P) or transurethral resection of the urinary bladder (TUR-M) operations, who were enrolled in a study to compare two intrathecal anaesthetics, 0.5% levobupivacaine (group L) and 0.5% bupivacaine (group B) (n = 100).
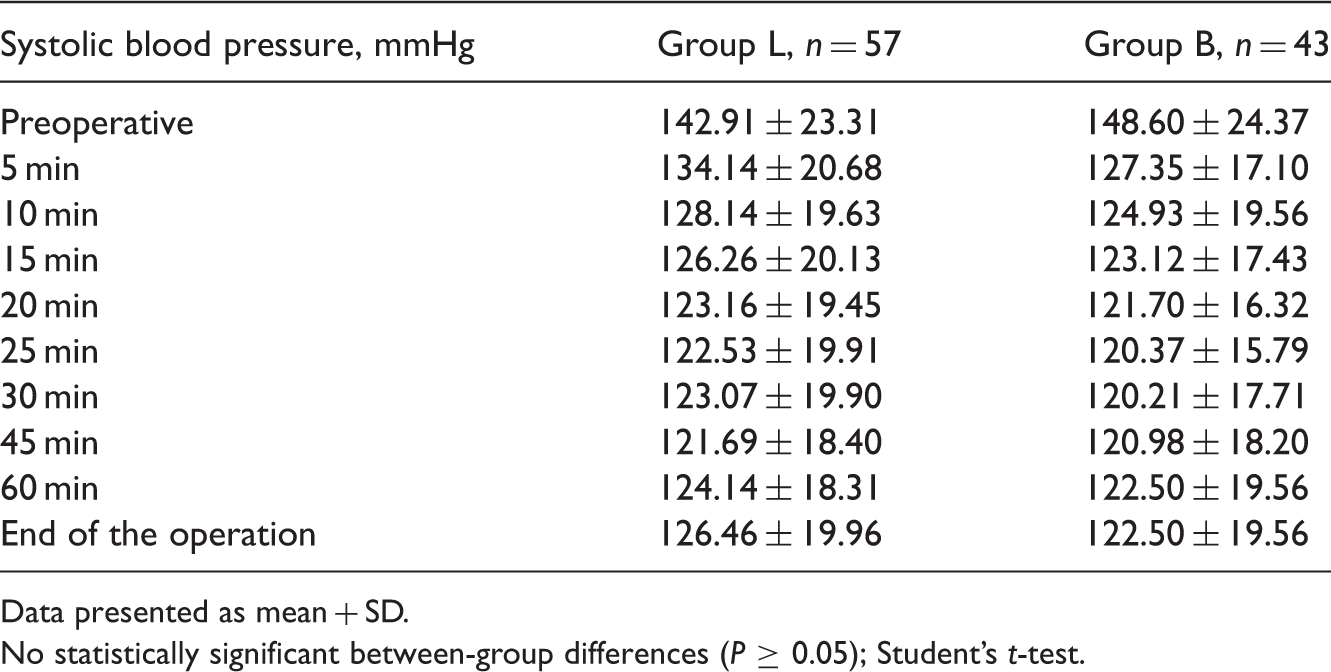
Data presented as mean + SD.
No statistically significant between-group differences (P ≥ 0.05); Student’s t-test.
Discussion
In this present study spinal anaesthesia was administered to patients aged
A prospective randomized double-blind study that compared the anaesthetic and haemodynamic effects of intrathecal levobupivacaine and bupivacaine demonstrated that levobupivacaine provided a faster increase in the Bromage score from 0 to 2 compared with bupivacaine, but there were no significant differences observed in any of the haemodynamic characteristics. 13 In contrast to these findings, 13 the present study showed that the time to onset of motor block was significantly faster with bupivacaine compared with levobupivacaine. Similarly, the time to onset of maximum motor block was significantly faster with bupivacaine compared with levobupivacaine in the present study.
In a study of intrathecally administered 3 ml (15 mg) of 0.5% levobupivacaine in 18 patients who were scheduled to undergo elective lower extremity surgeries, it was observed that the mean time to onset of sensory block was 3 min (range 2–10 min) and the mean time to onset of motor block was 5 min (range 2–10 min). 14 In this present study, the time to onset of sensory block and the time to onset motor block in patients treated with levobupivacaine were higher than in patients treated with bupivacaine. A randomized, double-blind study of spinal anaesthesia in 60 patients undergoing inguinal hernia repair that compared 8 mg hyperbaric 0.5% bupivacaine, 8 mg hyperbaric 0.5% levobupivacaine and 12 mg hyperbaric 0.5% ropivacaine found that the onset time and intraoperative efficacy of levobupivacaine and bupivacaine were similar. 15 In this present study of 15 mg hyperbaric bupivacaine compared with 15 mg isobaric levobupivacaine in patients undergoing TUR-P and TUR-M operations, the time to onset of motor block was significantly longer for patients treated with levobupivacaine and the motor block score only reached levels comparable with those of bupivacaine at 60 min after intrathecal injection.
In terms of haemodynamic parameters, a comparative study of healthy volunteers who were administered intravenous injections of levobupivacaine and bupivacaine reported that compared with their baseline values, both the stroke index and ejection fraction decreases were significantly smaller for levobupivacaine than bupivacaine; there was a smaller degree of prolongation in the PR interval with levobupivacaine than bupivacaine, but the difference was not statistically significant. 16 Hypotension is a very frequent side effect after spinal anaesthesia and it may cause serious increases in morbidity: it can even lead to mortality.4,17,18 In this present study, intravenous prehydration with 0.9% NaCl was given to all patients and saline infusions (0.9% NaCl at 4 ml/kg per h) were continued until the end of the operation; and there were no cases of hypotension that required intravenous ephedrine treatment.
It has been shown that the sympathetic nervous system-related side effects of levobupivacaine are less frequent than those associated with the use of bupivacaine and the mean convulsive dose for levobupivacaine is higher than that of bupivacaine.19,20 Previous animal studies reported that the possibility of causing convulsions or apnoea was lower with levobupivacaine than bupivacaine.19,21 Whereas several cases of central nervous system toxicity have been reported after intravascular injection of ropivacaine and levobupivacaine, no cases of serious cardiotoxicity or death have been reported in the literature.22–24 The clinical outcomes of levobupivacaine in children who underwent spinal anaesthesia were similar to those achieved with the same dose of bupivacaine. 25
A randomized, double-blind study of intrathecally administered 0.5% isobaric levobupivacaine or 0.5% hyperbaric bupivacaine in 70 patients scheduled to undergo elective transurethral endoscopic surgery found similar results between the two groups for the following variables: duration of sensory block, duration of two segment regression, time of onset and expiration of motor block, side effects, and pain scores at the beginning of the operation. 26 The authors suggested that 2.5 ml of 0.5% isobaric levobupivacaine and 0.5% hyperbaric bupivacaine provided the same clinical outcomes for spinal anaesthesia. 26
In this present study, there were no significant differences between levobupivacaine and bupivacaine in terms of the sensory block scores following intrathecal injection. A prospective, randomized, double-blind study conducted in 50 patients who underwent urogenital surgery found no statistically significant differences in the sensory and motor block properties, as well as the haemodynamic effects, of 0.5% levobupivacaine and 0.5% bupivacaine; the authors suggested that levobupivacaine was an effective substitute for 0.5% bupivacaine. 27 Although animal research has demonstrated that the duration of sensory and motor block was similar for levobupivacaine and bupivacaine, 19 there is some evidence of a small increase in duration of sensory block with levobupivacaine. 8 In contrast, there is also evidence that levobupivacaine is less potent than bupivacaine. 28
The sensory blocking effects of bupivacaine and levobupivacaine were similar according to these current findings. In the bupivacaine group, there was a relatively rapid regression of the sensory block level although the differences between time-points were not significant. Some clinical studies suggest that the local anaesthetic effects of levobupivacaine are different from those of bupivacaine. For example, in studies in patients undergoing caesarean section, intrathecal levobupivacaine was shown to have a similar clinical profile as bupivacaine, but it provided a lower level of motor block at the same dose.29,30 Good hemodynamic stability with a reduced prevalence of side effects has been shown for intrathecal levobupivacaine in elderly patients.31,32
In this present study, the haemodynamic, sensory and motor block effects of intrathecal levobupivacaine and bupivacaine injections were compared in 100 patients ≥65 years of age undergoing either TUR-P or TUR-M operations. Levobupivacaine did not cause any significant changes in haemodynamic parameters, and showed a similar sensory block onset time compared with bupivacaine, but it had a significantly longer motor block onset time compared with bupivacaine.
A limitation of the present study is the small number of patients in the groups. Further studies should be undertaken with a large number of patients to confirm the findings.
In conclusion, these current findings suggest that levobupivacaine can be used as a substitute for bupivacaine for spinal anaesthesia in elderly patients
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.