
Abstract
A pilomyxoid astrocytoma is a recently described tumor that occurs predominantly in the hypothalamic-chiasmatic region and is rarely found elsewhere. It has similar features as pilocytic astrocytomas, but has distinct histological characteristics and a poorer prognosis. A pilomyxoid astrocytoma is an aggressive tumor, and increased awareness is necessary with a suspect case. We present the first case of a pilomyxoid astrocytoma of the brainstem described after the newest World Health Organization classification of central nervous system tumors.
Introduction
A pilomyxoid astrocytoma (PMA) is a recently described brain tumor that has similar features as pilocytic astrocytomas (PAs), which are the most common central nervous system (CNS) tumor in the pediatric population. A PMA was included as a variant of PAs in the most recent World Health Organization (WHO) classification of CNS tumors, 1 and the WHO considers a PMA to be a grade 2 variant of PA with distinct histological characteristics and a poorer prognosis. Unlike PAs, the existence of PMAs in the brainstem is quite rare, according to the literature, as they occur predominantly in the hypothalamic-chiasmatic region.
Brainstem gliomas account for approximately 15% of pediatric CNS tumors. 2 They are heterogenous in clinical and pathological presentation and can be categorized as focal or diffuse tumors. The focal subtype represents 14% to 24% of the all brainstem gliomas and has a better prognosis than the diffuse subtype. 2 The most important goal in the surgical treatment of childhood brainstem tumors is achieving a gross total resection of the lesion. The malignant histological nature of the tumor is very important because this nature affects the prognosis, though not as significantly as the extent of tumor resection. 3
Case Report
Presentation
We present an 11-year-old female with an 8-month history of diplopia and progressive gait disturbance. Upon neurological examination, we found a Karnofsky Performance Status Scale (KPS) score of 70, a gait deviation to the left, an appendicular ataxia and palsy of the left abducens nerve. A magnetic resonance imaging (MRI) study and proton spectroscopy showed a pons-mesencephalic tumor consistent with a focal glioma (Figure 1).

Pre-operative magnetic resonance imaging of brainstem pilomyxoid astrocytoma (pre-contrast T1WI / T2WI, post-contrast T1WI).
Operative Procedure
The patient underwent a microsurgical resection by the telovelar approach of the fourth ventricle (prone position and midline suboccipital craniotomy). An ultrasonic aspirator was used to remove the tumor, and the evoked potentials of the brainstem were not available. Intraoperatively, after superior retraction of the cerebellar tonsils and vermis, we observed an exophytic tumor arising dorsally from the midbrain with a close relationship with the vessels of the brainstem; thus, a gross total resection was not considered safe.
Histological Examination
The following pathological features were observed: a cross-sectional view showed a typical pilomyxoid microcystic background with bipolar tumor cells, an angiocentric arrangement, and the absence of Rosenthal fibers and rare eosinophilic granular bodies (Figure 2). After deparaffinization, the histological slides were incubated with the appropriate monoclonal/polyclonal antibodies. The visualization of the reaction was performed using the avidin-biotin-peroxidase technique. The results of the immunohistochemical analysis are as follows: the glial fibrillary acidic protein was positive, the synaptophysin was negative and the Ki67 index was less than 10% (Figure 3). The histologic samples were reviewed by two neuropathologists.
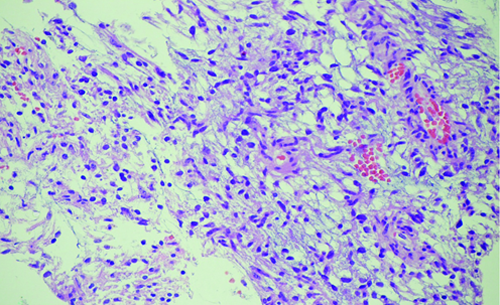
Typical histology of the pilomyxoid astrocytoma with myxoid matrix, lack of Rosenthal fibers and angiocentric arrangement.
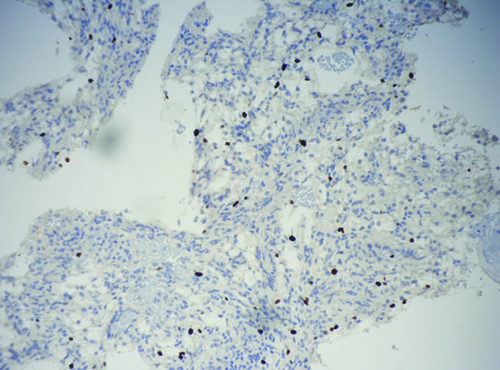
Photomicrograph showing Ki67 immunohistochemistry.
Postoperative Course and Treatment
The patient improved from the original symptoms, and the post-operative MRI showed a residual tumor. A repeat surgery was performed 9 months later due to neurological deterioration. Both operations resulted in a subtotal resection, but the patient's symptoms completely resolved. At 18 months post-operation, the patient was evaluated and given a KPS score of 90. A neuroaxis MRI found no evidence of disease dissemination. No adjuvant therapy was indicated until the present time. In view of the age of our patient, we believe that chemotherapy administered concomitantly with radiotherapy will be the best choice to prevent further progression. Our preferred regimen of chemotherapy is a combination of cisplatin (CCPD) and carboplatin (CBDCA).
Discussion
PMAs occur mainly in the pediatric population, but recent reports have indicated that PMAs can occur in adults. 4 Knowledge about this tumor is increasing, but PMAs arising from the posterior fossa have been rarely discussed in the neurosurgical literature. 5
PMAs belong to a group of low-grade astrocytomas and have recently been recognized as an entity (grade II WHO). They are differentiated histologically from pilocytic astrocytomas because of the lack of Rosenthal fibers and eosinophilic granular bodies.
Radiologically, PMAs are well circumscribed, may have solid or cystic components, are isointense on T1 and hyperintense on T2, which is enhanced homogeneously or heterogeneously after the injection of gadolinium. The ADC values and T2 signal intensity are generally higher than in PAs, which indicates the proportion of myxoid matrix. 6 No singular neuroimaging feature can reliably diagnose PMAs. 7
A computer search of the medical literature with the terms pilomyxoid astrocytoma, pediatric and brain tumor was performed to identify the relevant studies, published before September 2012, regarding PMAs of the brainstem.
We found five cases of PMAs of the brainstem in a series of 80 pediatric patients diagnosed with pilocytic astrocytomas by Fernandez et al.; 8 at the time of this study, there was no official distinction between PMAs and PAs. The lesions had pilomyxoid features, which were validated after 2007 by the World Health Organization. 1
In 2010, Johnson et al. 9 performed an extensive review of the medical records from three U.S institutions, examining a total of 84 cases. There were 42 PMAs and 42 intermediate tumors (a combination of pilomyxoid features and pilocytic qualities). There were two intermediate tumors of the brainstem and no pure PMAs. The 84 cases included a series of 18 patients published by Tihan et al. 10 in 1999. Other smaller series and case reports indicated as having an unusual presentation have been reported, but no cases of PMA in the brainstem were found.
To evaluate the prognostic factors in pediatric brainstem gliomas, Albright et al. 3 reviewed the charts of 84 children; the biopsy data were available in 54 cases. The tumors were broadly classified into two categories: low-grade (benign) and high-grade (malignant). After analyzing the histological features, the authors observed that the biopsy specimens with calcification and Rosenthal fibers were related to a better prognosis, while the presence of mitoses indicated malignancy; all 18 patients in whom mitoses were observed died. Most cases were classified as benign gliomas with no pathological characteristics suggesting PMA.
In our patient, a rapid regrowth of the brainstem tumor occurred in a few months, which is characteristic of an aggressive tumor. The results of our histological examination were identical to those observed in the classic hypothalamic/chiasmatic PMAs, i.e., monophasic architecture with a myxoid background and the absence of Rosenthal fibers.
The management of PMA remains controversial, and there is no consensus. There is a tendency to recommend adjuvant therapy (i.e., chemotherapy or radiotherapy) in cases of tumor recurrence or partial resection. 11 The gross total resection of the tumor is the most reliable predictor of a favorable outcome. Advances in refining molecular therapy that are obtained with a better understanding of glioma pathogenesis are promising. In view of the significant trend of regrowth and cerebrospinal fluid (CSF) spread, a strict follow-up is recommended. 12
Conclusions
Though most PMAs occur in the hypothalamic region, lesions in unusual locations should be noted to expand the current epidemiologically known locations for this tumor. To our knowledge, our study identified only the sixth case of pilomyxoid astrocytoma located in the brainstem, and it was the first published case after the WHO classification of 2007.
The efforts towards PMA registries should be encouraged because the creation of a database will help neurosurgeons and pediatric neuro-oncologists better understand this disease and allow for more reasonable decisions about surgical and medical treatments based on the aggressive biological behavior of the tumor.
Footnotes
Conflict of interests: the authors declare no potential conflict of interests.