
Abstract
Myxofibrosarcoma (MFS) is a variant of the group of malignant fibrous histiocytomas. It is one of the most aggressive types of soft tissue neoplasms. The clinical presentation is not pathognomonic and the histological aspects are highly heterogenous, frequently delaying the diagnosis or leading to misdiagnosis. Complementary histochemical and immunohistochemical stainings are mandatory to achieve the diagnosis of MFS. A 78-year-old male patient is presented illustrating this diagnostic pitfall. Extensive surgery followed by radiotherapy is the first choice treatment.
Introduction
Malignant fibrous histiocytoma (MFH) belongs to the heterogeneous group of fibrohistiocytic tumors.1–4 MHF is part of soft tissue neoplasms, composed of cells sharing fibroblastic and histiocytic features. MFH is one of the most aggressive of the group of fibrohistiocytic tumors. MFH exhibits a high local recurrence rate and a significant metastatic rate. It is also the most frequent sarcoma found in the adult patient.
Case Report
A 78-year-old man, without any remarkable medical or surgical history, presented an asymptomatic, rapidly growing, indurated and firm nodule on the right forearm. Over two months, the lesion had reached about 4 cm in diameter (Figure 1). There was no previous skin lesion and the site was never traumatized or irradiated. A differential diagnosis of a cutaneous metastatic lesion or a kystic lesion was suggested. Surgical excision was performed under local anesthesia with tumor removal until the muscular fascia. The histopathologic picture showed a well-defined, well-limited large nodular lesion located in the subcutaneous fat tissue composed of a dense pleomorphic-storiform cellular infiltrate. There were numerous round, fusiform and stellate tumor cells with undefined cell margins, eosinophilic cytoplasms and hyperchromatic atypical nuclei. Immunohistochemical staining revealed that the tumor cells were positive for vimentin and p63, but negative for CK-7 (low molecular-weight cytokeratins), CK-20 (high molecular-weight cytokeratins), CD117, actin, protein S100a and HMB45, suggesting a metastatic adenocarcinoma. The deep surgical margins were free of tumor involvement.

Primary tumoral lesion on the right forearm.
The patient was hospitalized for searching the initial tumor. A total body scan, a PETscanner and an extensive blood test were all negative. Tumor markers were negative. IRM imaging of the involved arm revealed no residual tumor or further tissue invasion. Facing the absence of a primary tumor, a second opinion on the histology of the initial tumor tissue was requested. Other immunohistochemical markers revealed a strong positive signal for CD99 and alpha-anti-trypsin whereas desmin, pancytokeratin, EMA, CD68 and factor XIII-a remained negative. These findings were suggestive of MFH. Furthermore, the presence of extensive myxoid matrix changes containing elongated curvilinear capillaries (Figures 2 and 3) as revealed by the PAS-iron colloidal histochemical stain favored a diagnosis of a myxoid variant of MFH, also called myxofibrosarcoma (MFS).

Histologic examination of the primary lesion (Haematoxylin and Eosin, x 20).
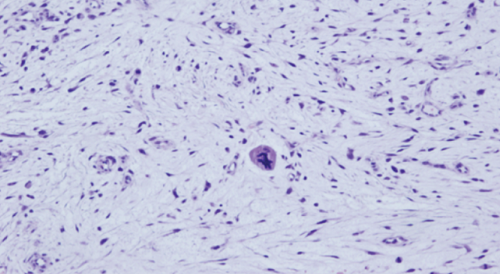
Histologic examination of the primary lesion (Haematoxylin and Eosin, x 40).
As the surgical margins were free of tumor involvement and as the IRM imaging presented no further particularities, the pluridisciplinar cutaneous oncology group recommended strict clinical surveillance but no complementary radiotherapy.
Three months later, at a control visit, the patient presented two new smaller asymptomatic firm nodular lesions in the immediate vicinity of the previous surgical scar (Figure 4). These lesions were again surgically removed under local anesthesia. Histology revealed again a myxoid variant of MFH. There was an invasion of the deep surgical margins. Subsequently, a large surgical reexcision was performed including removal of the fascia. A PETSCAN excluded the presence of suspect locoregional lymphadenopathies. Du to the rapid occurrence of the MFS recurrence, it was decided to perform complementary radiotherapy (25 sessions). Up to date, the patient is recurrence free and has no functional disability of his arm.

Two small recurring lesions adjacent to the initial surgical excision.
Discussion and Conclusions
Fibrohistiocytic tumors represent a highly heterogeneous group of soft tissue neoplasms composed of cells exhibiting fibroblastic and histiocytic features.1,3,5 MFH is one of the most common soft tissue tumors in adult patients.1,3,6 MFH also exhibits a very aggressive loco-regional behavior, with a high risk for local recurrence and a significant metastatic rate. 4 MFH is usually classified as superficial or deep tumor. The superficial variant typically presents as a painless, progressively enlarging single nodule. Tumor growth may occur over several months, sometimes reaching 5 to 10 cm in size at the time of diagnosis. Superficial MFH is also known as atypical fibroxanthoma. It shows a more favorable prognosis than others type. Any area of the body may be involved but the most common sites are the extremities.
Several other subtypes of MFH are described in the literature including the pleomorphic, the myxoid, the giant cell, the inflammatory and the angiomatoid variants. The myxoid type, also known as myxofibrosarcoma (MFS), is the second most frequent subtype, representing approximately 20% of cases and is characterized by an association of myxoid areas and cellular areas in variable proportions. 7–9 They are among the most frequent malignant mesenchymal tumors of the elderly.4,8,9 The mean age is 66 years and the sex ratio is 1:1.4 The extremities are the most common site followed by the trunk, the pelvis, the head and neck region and the genital area. 4 The most frequent initial presentation is a single cutaneous asymptomatic nodule. 10 The deep dermis and hypodermis are the preferential sites and represent about 2/3 of the cases of MFS. The abundance of myxoid areas defines the lesion's grade, being more prominent in lower-grade lesions. The differential diagnosis should exclude benign myxoid neoplasms, epitheloid types of MFS, carcinoma, melanoma, myoepithelial carcinoma, pleomorphic liposarcoma and pleomorphic rabdomyosarcoma. 11
As illustrated in this case, not only the clinical diagnosis but also the histopathologic identification can be very difficult. 8 One paper related 3 cases of myxofibrosarcoma that were initiallyl diagnosed as benign cutaneous neoplasms. 8 Final diagnosis relies on a large series of histochemical and immunohistochemical staining.11,12 Immunohistochemistry typically stains positive for only vimentin and occasionally actin. 12 DNA flow cytometry reveals an association between aneuploidy and histologic grading. Local recurrence occurs in about 50% of the patients with MFS. Distant metastasis occurred in 13/60 patients and death was attributed to MFS in 13/60 cases.4 Metastasis only occurred in patients exhibiting intermediate or high grade MFS. MFS typically behaves more aggressively if recurrent lesions appear. 4
Large resection represents the first choice of treatment.4,8 Surgical excision has to be as large as possible as MFH may spread over a considerable distance beyond the gross tumor margins. Insufficient tumor-free margins are the open door to local recurrence, and hence a worse prognosis.
Due to the high recurrence and metastatic rate of MFH, adjuvant radiation therapy is recommended to treat eventual occult local micro metastases. Metastatic sites are essentially pulmonary and lymphatic.
The prognosis of MFH seems to correlate with four principal features. The increasing depth of tumor invasion is the most predictive for the risk of metastatic disease. The size of the tumor (smaller than 5 cm versus greater than 5 cm), the anatomical location (distally versus proximally located tumors) and the histological features (including the degree of anaplasia and the number of mitoses) also correlate with prognosis.4,8
The follow-up of MFS patients should be very thorough to manage properly eventual local recurrences.
In conclusion, MFH is a great clinical mimicker and may present a histologic nightmare. A large series of histochemical and immunohistochemical stainings is recommended. Extensive surgical excision with adjuvant radiotherapy presents the optimal therapeutic option.
Footnotes
Conflict of interests: the authors declare no potential conflict of interests.