
Abstract
Nephrogenic adenoma (NA) is an uncommon benign lesion of the urothelial tract. The diagnostic features that are useful in the recognition of this benign entity are: the characteristic mixture of various architectural patterns, associated stromal edema and inflammation, hyaline sheath around tubules, and lack of mitotic activity. Although NA appears with hematuria or obstruction, frequently found incidentally in endoscopy or imaging modalities.
Introduction
Nephrogenic adenoma (NA) is a rare metaplastic lesion of the ureter. It is assumed to be secondary to chronic irritation of the urothelium. Although it can be seen anywhere in the urinary tract, it is most commonly observed in the bladder (55%). The incidence in ureter is approximately 4%. 1 Firstly, it was defined by Davis with the name hamartoma. 2 Later it was named nephrogenic adenoma because of the tubular structures in the lesion. 3 Although nearly 300 cases have been reported in the literature, lower than 20 of them affected the ureter. We report here a case of a young woman having incidental lesion and review the literature.
Case Report
A 28 years old female patient was admitted to our clinic with left flank pain. Approximately 6–8 mm urinary stone was observed at the left midureter in intravenous pyelograhy (Figure 1). Spiral computed tomography confirmed the urinary stone at the same localization. As the left flank pain was severe and lasted approximately for one week, the patient was scheduled for left ureterorenoscopy. A polypoid structure at 10 cm in left ureter was observed during ureterorenoscopy. The stone just behind this polypoid structure was broken with pneumatic lithotripter and removed with basket catheter. Polypoid structure was cut totally with the cold knife during ureterorenoscopy. A double-J catheter was placed to the patient at the end of procedure and removed one month after. After the removal of the stent, there was no stricture of the ureter.
Intravenous pyelograhy demonstrating an obstruction (arrow) of the left midureter.
Histologically, the lesion is lined by hobnail cells consisted of papillary and tubular structures (Figure 2). Inflammatory cell infiltration in the surrounding lamina propria, edema and vascular structures were observed. The lesion stained diffusely with low-molecular-weight cytokeratin, cytokeratin 7 (CK7) and epithelial membrane antigen (EMA) in immunohistochemical staining (Figure 3). P53 and p63 staining was not observed (Figure 4).
Nephrogenic adenoma. Tubules and papillary fronds lined by hobnail cells (Hmatoxylin and Eosin × 40).
Immunhistochemically the lesion was diffusely positive for low molecular weight cytokeratin (A) positive for epithelial membrane antigen (B) positive for CK7 (C).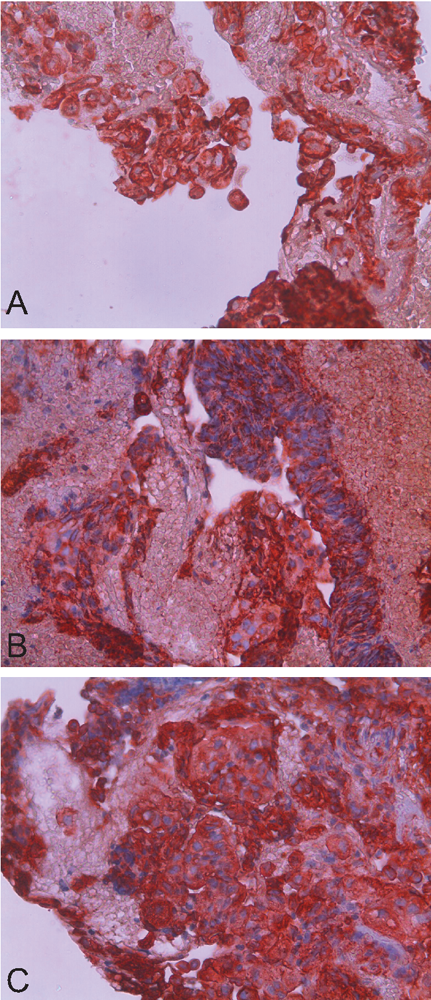
Immunhistochemically the lesion was negative for p53 (A) and negative for p63 (B).
Discussion and Conclusions
NA, which is more common in men than in women (male to female ratio 2:1), is a rare benign lesion of the urothelium.4,5 The most common clinical presentations of NA are: previous surgery, trauma, chronic urinary tract infections, and/or recurrent urolithiasis.1,4 Although NA appears with hematuria or obstruction, it is frequently found incidentally in endoscopy or imaging modalities. 6 It may mimic malignancy radiologically with mass image and filling defect. Majority of NA are lower than 1 cm and it rarely grows up to more than 7 cm. 7 NA has a high rate of local recurrence but malignant transformation has not been reported until now.
Patients may appear with massive hematuria, dysuria, nocturia, urinary frequency, renal colic, and microhematuria. Sometimes it can also be detected incidentally in nephrectomy and nephroureterectomy specimens. 8 Today NA is considered to be a secondary metaplastic response of the urothelium to chronic irritation. Although it can be seen anywhere in the urinary tract, it is most commonly seen in the bladder (55%) followed by urethra (41%) and ureters (4%) respectively. 4
Kaswick et al. suggested the two main theories as embryological and inflammatory theory related to pathogenesis. Embryological theory is not descriptive for lesions out of trigone. However, inflammatory theory defined as metaplastic response of urothelium to chronic inflammation and irritation remains valid. 9
Histologically, nephrogenic adenoma may presents in different patterns showing tubular, cystic, papillary and solid growth pattern. The most common form is a tubular structure surrounded by a thick hyalinized basal membrane. It consists of clear cells without apparent nucleolus or cubic cells with eosinophilic cytoplasm or hobnail cells. Edema, acute and chronic inflammation in stroma is common. NA is typically stained positive with cytokeratin 7 (CK7), PAX2, α-methylacyl-CoA race-mase (AMACR) (P504S) and EMA. It is usually not stained with p63 and p53.10 Absence of cytological atypia, high mitotic activity, necrosis, and absence of p53 staining excludes malignancy. Our patient was diagnosed with NA because of the absence of histomorphological nuclear atypia, mitosis, solid tumor islands and the presence of benign-looking hobnail cells forming characteristic tubular structures in edematous and inflamed stroma. The lesion in our case stained diffusely with CK7, EMA and low-molecular-weight cytokeratin but not with P53 and p63. As a result, ureteral NA is a rare benign lesion and the diagnosis is important as it may mimic malignancy. Malignant transformation has not been described to date however it must be followed up for probable local recurrences.