
Abstract
Meningeal metastasis is rare in the clinical course of ovarian carcinoma and its prognosis is extremely poor. We experienced a case of carcinomatous meningitis from metastatic ovarian small cell carcinoma. A 33-year-old woman with atypical genital bleeding, was diagnosed with a right ovarian tumor and referred to our department. She underwent a total abdominal hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and lymphadenectomy. It was an optimal debulking surgery. She was diagnosed with ovarian carcinoma classified as Stage IIIc according to the Féderation Internationale de Gynécologie et d'Obstétrique classification system. Histological findings showed small cell carcinoma of the pulmonary type. The tumor was bilateral with paraaortic lymph node involvement. The patient was treated with irinotecan and cisplatin (CPT-P therapy). After 4 courses of CPT-P therapy, multiple liver metastases and Virchow's lymph node metastases were found. She was treated with amrubicin as a second-line chemotherapy, but the treatment was ineffective. Five months after surgery, the patient complained of severe headache and nausea. Lumbar puncture was performed and cytology was positive. Magnetic resonance brain imaging indicated meningeal thickening. The patient was diagnosed with meningeal metastasis and received 19-Gy whole cranial irradiation. In spite of these treatments, her disease progressed rapidly and she was often drowsy. She died of aspiration pneumonia 6 months after surgery.
Introduction
The occurrence of carcinomatous meningitis (CM) seems to have increased with improvements in antineoplastic treatments, and 5–8% of patients with malignancy suffer this complication.1–6 The primary cancers associated with this condition include breast cancer, lung cancer, melanoma and the lymphomas and leukemias.1–4,7 The therapeutic management of CM remains controversial and no straightforward guidelines can be found in the literature.1,2 Ovarian small cell carcinoma is extremely rare. It is extremely aggressive and progressive, and there are no established treatment protocols.4,8–14 Here, we report a rare case of ovarian small cell carcinoma complicated by CM.
Case Report
A 33-year-old Japanese woman (gravida 1, para 1) was referred to our hospital with abdominal pain and atypical genital bleeding. Ultrasonography revealed a large pelvic tumor without ascites. Computed tomography (CT) scanning and magnetic resonance imaging (MRI) revealed a large right ovarian tumor (95×83×142 mm) and pelvic and paraaortic lymph node metastasis (Figure 1).
Magnetic resonance imaging findings. A) Pelvic T2-weighted imaging (WI), sagittal; B) Pelvic T2-WI, transverse. There was a large tumor (95×83×142 mm) on the right side of the pelvic cavity. There were few ascites and no evidence of tumor invasion to the surrounding tissue.
The serum levels of tumor markers were as follows: neuron-specific enolase, 39.1 ng/mL (normal range: <10 ng/mL); pro gastrin-releasing peptide, 52 pg/mL (normal range: <46.0 pg/mL); squamous cell carcinoma antigen, 0.5 ng/mL (normal range: 1.5 ng/mL); carcinoembryonic antigen, 82.7ng/mL (normal range: 0–5 ng/mL); cancer antigen 19–9, 3.3 U/mL (normal range: 0–37.0 U/mL); CA125, 48.9 U/mL (normal range: <35.0 U/mL); CA72–4, 3.0 U/mL (normal range: <4.0 U/mL); alpha fetoprotein, 3.1 ng/mL (normal range: 0–13.5 ng/mL).
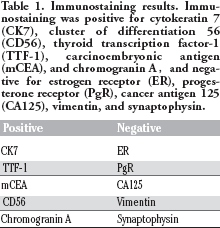
Ovarian cancer was suspected, and the patient underwent debulking surgery, including total hysterectomy with bilateral salpingo-oophorectomy, omentectomy, pelvic lymphadenectomy and paraaortic lymphadenectomy at our hospital (Figure 2). The pathological diagnosis was a small cell carcinoma of the pulmonary type (Figure 3). Table 1 shows the immunohistochemical results. There were no evidences of lung cancer (pulmonary tumors or enlarged mediastinal lymph nodes) by CT scanning. So, we diagnosed primary ovarian cancer Stage IIIc according to the Féderation Internationale de Gynécologie et d'Obstétrique (FIGO) classification system, involving the bilateral salpinxes and ovaries, and pelvic and paraaortic lymph nodes. At 2 weeks after operation, the patient received first-line chemotherapy combining cisplatin (60 mg/m2, Day 1), and irinotecan (60 mg/m2, Day 1, 8, 15) CPT-P therapy) administered every 4 weeks by intravenous infusion. After 4 courses of this regimen, multiple liver metastases and Virchow's lymph node metastasis were found on CT. The patient then received second-line chemotherapy using amrubicin (45 mg/m2, Days 1, 2, 3) beginning 5 months after surgery. Around the same time, she began to complain of headache. Brain MRI was carried out, but there were no remarkable findings. Nevertheless, the patient's headache worsened and she also complained of a stiff neck. She tested positive for meningeal irritation, and an examination of cerebrospinal fluid (CSF) was performed. Cytological examination showed small cell carcinoma cells (Figure 4). The patient was thus diagnosed with CM at 5 months after surgery. Brain MRI was performed again and showed remarkable CM. The patient gradually became less aware of her surroundings, and her headache and vomiting worsened. Although she received whole brain irradiation (19Gy), it was not effective. She contracted pneumonia, and died 6 months after her first surgery.
Cross section of the tumors in the right ovary. The tumor was the size of the new born child head, and weighted 1,500 g. It was gray-white in color and solid, with necrotic lesions.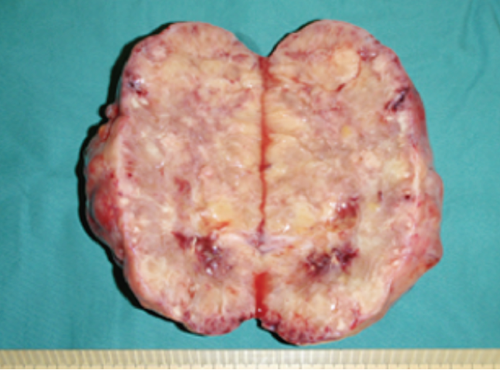
Histological findings of the right ovary. The tumor was densely cellular and was arranged in sheets, closely packed nests and rosette formation. The tumor cells had scanty cytoplasm and small to medium-sized hyperchromatic nuclei that were oval to spindle shaped. A) Hematoxylin and eosin, original magnification ×100; B) hematoxylin and eosin, original magnification ×100; C) hematoxylin and eosin, original magnification,×200; D) Hematoxylin and eosin, original magnification ×400.
Immunostaining results. Immunostaining was positive for cytokeratin 7 (CK7), cluster of differentiation 56 (CD56), thyroid transcription factor-1 (TTF-1), carcinoembryonic antigen (mCEA), and chromogranin A, and negative for estrogen receptor (ER), progesterone receptor (PgR), cancer antigen 125 (CA125), vimentin, and synaptophysin.
Cytological specimens from the spinal fluid by lumbar puncture. The tumor cells had scanty cytoplasm and hyperchromatic nuclei and were similar to small cell carcinoma cells. There were paired cells grouped to form a line. A,B) May-Giemsa staining, original magnification ×400.
Discussion
Primary ovarian small cell carcinoma of the pulmonary type is extremely rare. 9 It resembles small cell carcinoma of the lung. 15 Eichhorn et al. report 11 patients ranging in age from 28 to 85 (mean 59) years of age with primary ovarian small cell carcinoma of the pulmonary type. 9 In the long-term follow-up, they died of the disease at 1–13 (mean 8) months.
CM is diagnosed in 1–8%, (1,2,4,6) of patients with solid tumors and in 5–15% of patients with leukemia. 1 The incidence of CM is increasing as imaging studies have improved and as cancer patients have begun to live longer.2,4,5 The incidence of CM is 5% in non-small cell lung cancers, and 5% in breast cancer.1,4,5 In small cell lung cancer, the incidence of CM is 9–25%.1,4 Central nervous system (CNS) metastasis from ovarian carcinoma is rare.3,7,16–19 The incidence of CM with ovarian cancer is 0.08–0.28%. 20 In Eichhorn's report on primary ovarian small cell carcinoma of the pulmonary type, 1 of the 11 patients (9%) had brain and spine metastases. 9 The median survival time of untreated patients with CM is 4–6 weeks.1,5,21 Patients with CM typically die of progressive neurological dysfunction. 1
The most common way of diagnosing CM is by positive cytology upon CSF examination and/or radiological studies. However, CSF cytology is low sensitivity. In patients with positive CSF cytology, 45% are cytologically negative on initial examination.1,2,5 In neuroradiographics studies, MRI with gadolinium enhancement (MR-Gd) is better than enhanced CT scanning. The sensitivity of MRI is nearly 70% while that of CT scanning is about 30%.1,2,5
There are no standard treatments for CM. In most cases, chemotherapy and radiotherapy have been used in different modalities.1,5 Chemotherapy has been given systemically, intrathecally via lumbar puncture and intra-ventricularly via an Ommaya reservoir.2,5 Most patients with CM have metastatic disease, and are usually treated systemically. 5 Intrathecal chemotherapy is the mainstay of treatment for CM patients. Retrospective analysis or comparison with historical series suggests that the administration of chemotherapy to the CSF improves the outcome of patients with CM.1 For intrathecal and intraventricular administration, 3 agents are routinely used: methotrexate, cytarabine and thiotepa. To the best our knowledge, no difference in response has been reported among single-agent methotrexate with thiotepa or multiple-agent (methotrexate, thiotepa, and cytarabine or methotrexate and cytarabine) versus single-agent methotrexate treatment.1,5
Radiotherapy is used in the treatment of CM for palliation of symptoms, decreasing bulky disease and the correction of CSF flow abnormalities demonstrated by radionuclide ventriculography. 1 Whole neuraxis irradiation is associated with significant systemic toxicity (severe myelosuppression and mucositis among other complications) and has not been reported to be curative. 1
Since our patient suffered from CM and multiple organ metastases, we chose systemic chemotherapy and whole brain irradiation. The treatment recommendations of small cell carcinoma of the ovary are not conclusive;9,14 however, chemotherapeutic agents have been shown to be most effective against small cell carcinoma of the lung. 9 Eichhorn et al. reported a long-term survivor with stage IIIc ovarian small cell carcinoma of the pulmonary type; the patient underwent abdominal total hysterectomy, bilateral salpingo-oophorectomy, and retroperitoneal lymph node dissection and received chemotherapy including cyclophosphamide, cisplatin, doxorubicin, etoposide, and vincristine. 9 In the analysis of small cell carcinoma of the ovary of the hypercalcemic type, a chemotherapeutic regimen including etoposide, cisplatin/carboplatin or vinca alkaloids has been found to be associated with improved of patient survival. 10 In the present case, we chose a chemotherapeutic regimen including irinotecan/cisplatin and amrubicin, which are currently used for small cell lung cancer and are considered to be effective for small cell carcinoma of the ovary.9,22–25
Conclusions
In conclusion, we report here the extremely rare case of CM with primary ovarian small cell carcinoma. If ovarian cancer patients have severe headache or neck stiffness, the rare complication of CM should be considered.