
Abstract
Bronchogenic cysts are mostly benign, congenital abnormalities originating from the remnants of the primitive foregut. A retroperitoneal location is rare. Due to the mostly asymptomatic behavior and the historical confusion regarding histology, an exact prevalence is not known. We present here a case report of a retroperitoneal bronchogenic cyst. A literature review was performed for cases of retroperitoneal bronchogenic cysts written in English. Anatomopathological criteria for inclusion were pseudo stratified, ciliated, columnar epithelium together with the presence of at least one of the following: cartilage, smooth muscle or seromucous glands. In addition, the embryology, pathogenesis, radiological, clinical and suggested treatment modalities are reviewed. We report the surgical excision of a retroperitoneal bronchogenic cyst that presented as a non-functioning left adrenal mass. Our review of literature revealed only 62 potential cases of retroperitoneal bronchogenic cysts. After applying the strict anatomopathological criteria, only 30 cases of true retroperitoneal bronchogenic cysts could be identified. Retroperitoneal location of a bronchogenic cyst is rare. Despite the rarity of this pathologic entity, bronchogenic cysts should be considered in the differential diagnosis of retroperitoneal cystic lesions. Only histology can confirm definitive diagnosis. Surgery remains the recommended treatment of choice.
Introduction
Bronchogenic cysts originate from the tracheobronchial bud which arises at the embryonic foregut. 1 These lesions can be found in or near any organ derived from this embryonic foregut. Most frequently, they are encountered in the thoracic cavity, especially in the mediastinum, posterior to the carina or embedded in the pulmonary parenchyma.1,2 More distant locations have been reported such as skin,3–6 left ventricle, 7 intra-abdominal8,9 and retroperitoneal.9–35 Based on anatomopathological criteria, cysts arising from the primitive foregut can be classified as bronchogenic, enterogeneous (oesophageal and gastroenteric) or undifferentiated.20,27,36 Retroperitoneal localized bronchogenic cysts, as first reported by Miller et al in 1953, are very rare. 37 The preoperative diagnosis of retroperitoneal bronchogenic cysts remains challenging since there are no specific imaging features. The finding of a retroperitoneal cystic or solid lesion yields other, more common diagnoses.
The aim of this manuscript is to present a case report of a retroperitoneal bronchogenic cyst and to review its radiological, clinical and anatomopathological characteristics.
Case Report
A 48-year-old Caucasian male consulted the cardiologists with aspecific thoracic discomfort. Clinical examination revealed no abnormalities. Further radiological exploration by means of ultrasound (US), computed tomography (CT) and magnetic resonance imaging (MRI) revealed a multilocular left adrenal mass. (Figure 1) The lesion did not sign on positron emission tomography (PET) scan.
Magnetic resonance imaging of the retroperitoneal bronchogenic cyst T2 weighted (HASTE TE=60 m/sec) image in the coronal plane demonstrating a multilocular mass in the retroperitoneum on the left side. High and intermediate signal intensities (arrows) are demonstrated in the different loculi. The lesion is abutting from the upper pole of the left kidney.
Surgical excision of the retroperitoneal mass, en bloc with the left adrenal gland and a part of the left diaphragmatic crus, was performed through a left subcostal incision. Postoperative stay was uneventful. Macroscopic examination showed a multicystic, rubbery, brownish lesion, adhering to the left adrenal gland and left paraspinal diaphragmatic muscle fibers. The specimen weighed 58 g and measured 7×7,5×4,3 cm. Cross section revealed a lesion with a diameter of 4,5 cm located between a fragment of the diaphragm and a macroscopically normal adrenal gland. The lesion consisted of cysts with diameters ranging from 0,6 to 2,5 cm, filled with mucoid or gelatinous material (Figure 2).
Macroscopic view of a cross section of the retroperitoneal bronchoigenic cyst. A multicystic lesion located between the adrenal (A) and the diaphragm (D, marked with a suture).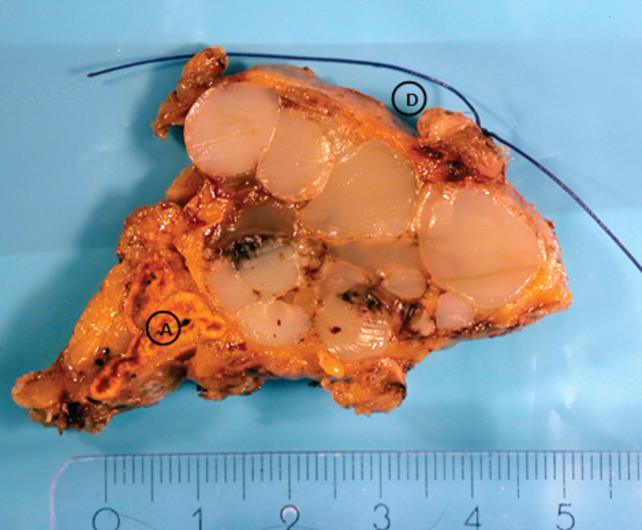
On microscopic examination the fragment of the diaphragm and the adrenal were normal. The cysts were lined by ciliated, columnar respiratory-type epithelium. In between, seromucous acini and some islands of cartilage were present. In addition, some alveolar-like structures were noted (Figure 3). The lining epithelium of het cysts was immunoreactive for cytokeratin 7 but negative for cytokeratin 20. The alveoli showed nuclear immunoreactivity for TTF-1 (a transcription factor present in lung and thyroid) (Figure 4). The lesion was diagnosed as a bronchogenic cyst.
Microscopic view (hematoxylineosin, ×5) of the retroperitoneal bronchogenic cyst. Cystic spaces lined by columnar epithelium (arrowheads), cartilage (C) and mucoid acini (arrow).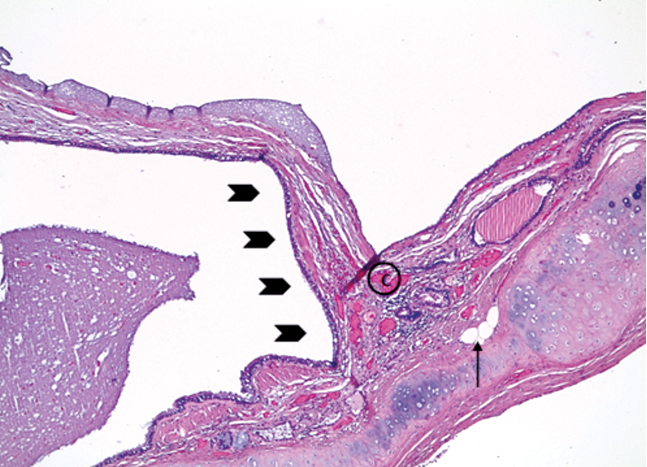
A microscopic view of the retroperitoneal bronchogenic cyst: spaces lined by epithelium showing nuclear immunoreactivity for the transcription factor TTF-1 (nuclei showing as round brown dots, ×10).
Literature review
A thorough literature review using the keywords retroperitoneal, bronchogenic and cyst was performed. PubMed and Embase were searched for literature written in English. All papers were reviewed with special attention to histological features. Bronchogenic cysts were defined by the following criteria: pseudo stratified, ciliated, columnar epithelium together with the presence of at least one of the following: cartilage, smooth muscle or seromucous glands.1,20
Results
Our search of MEDLINE revealed 62 cases of retroperitoneal bronchogenic cysts published worldwide, of which 46 were reported in English. After reviewing title and abstract, only 32 of these publications were retained. Figure 5 illustrates the search process. Subsequent critical appraisal of the full text articles, focused on the anatomopathological features, eventually yielded 27 publications reporting on 30 cases of true retroperitoneal bronchogenic cysts. Table 1 provides a concise overview of the included articles.
Literature review process.
All 30 Full text articles in english literature concerning bronchogenic cyst.
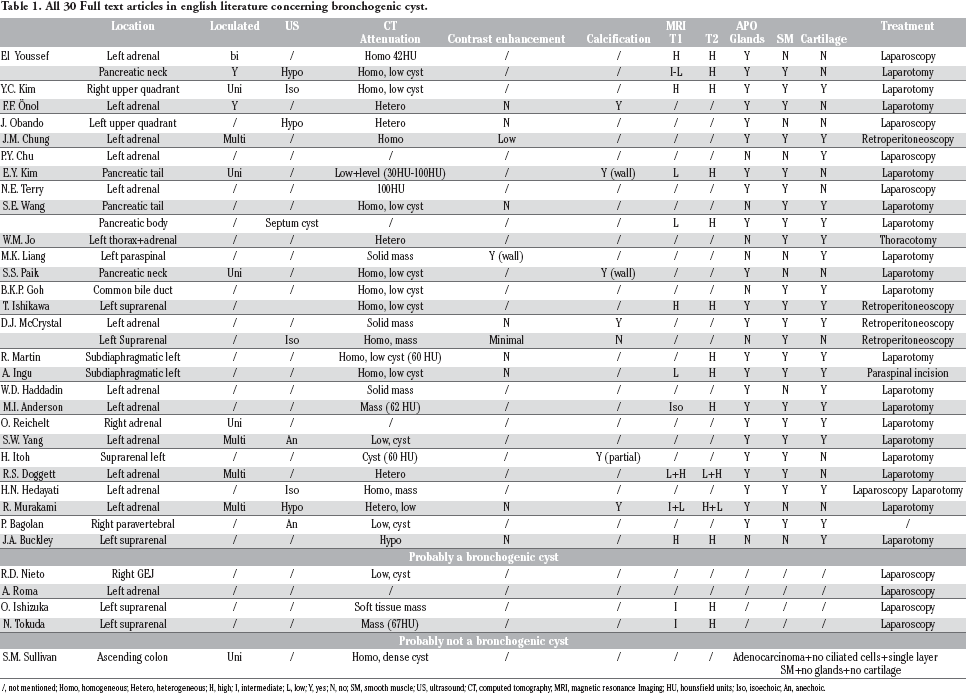
/, not mentioned; Homo, homogeneous; Hetero, heterogeneous; H, high; I, intermediate; L, low; Y, yes; N, no; SM, smooth muscle; US, ultrasound; CT, computed tomography; MRI, magnetic resonance Imaging; HU, hounsfield units; Iso, isoechoic; An, anechoic.
Discussion
Meyer et al. in 1859 were the first to report a case of a bronchogenic cyst. 38 No earlier than 1953, Miller et al. published about their possible retroperitoneal occurrence. 37 In the past, confusion regarding histological criteria has lead to misclassification of bronchogenic cysts. This provides an explanation for the discrepancy in reported cases between our first and further thorough literature search.
Embryology and pathogenesis
The exact pathogenesis of retroperitoneal localized bronchogenic cysts is still unknown. In order to understand suggested hypotheses regarding this location, the embryological development of three entities needs to be considered: the foregut (and its derivatives), the diaphragm and the retroperitoneal space.39,40 During the third and fourth week of embryogenesis, folding of a flat trilaminar (endo-, meso- and ectoderm) germ disc results into the formation of an elongated cylinder (Figures 6A–C). The central, endodermal tube constitutes the primitive gut tube. In relation to the boundaries of vascularisation of the future gastrointestinal tract, this primitive gut tube can be divided into foregut, midgut and hindgut. In the fourth and fifth week, an out-pouching; the respiratory diverticulum, appears on the ventral aspect of the future pharynx. Two laryngotracheal ridges form and fuse between this diverticulum and the dorsally located foregut, finalizing the tracheoe-sophageal septum. This structure divides the ventral respiratory laryngotracheal tube from the dorsal oesophagus. Next, a primitive lung bud develops at the caudal end of the laryngotracheal tube and starts growing ventrocaudally through the mesenchyme. By the end of the seventh week it divides into two bronchopulmonary buds, the precursors of the right and left lung.41,42
The future intraperitoneal cavity or coelom is formed when the mesoderm splits into two layers: the somatopleuric mesoderm (adherent to the ectoderm) and the splanchnopleuric mesoderm (adherent to the endoderm). Initially, the gut tube is attached to the dorsal body wall, covered by the splanchnopleuric mesoderm. During the fourth week, a bilayered dorsal mesentery originates from the splanchnopleuric mesoderm, which suspends the gut tube and its derivatives in the coelomic cavity (Figure 6D). This way, the future intraperitoneal viscera are formed in contrast to the retroperitoneal organs, that further develop in the dorsal body wall. Some parts of the gut tube that are originally suspended in the coelomic cavity eventually re-fuse with the dorsal body wall and, in doing so, become secondarily retroperitoneal. 41
The diaphragm starts forming in the fourth or fifth week of embryogenesis. First, the septum transversum appears, separating the primitive coelomic cavity into thoracic and abdominal portions. This is a transverse mesenchymal partition, attached ventero-laterally to the body wall and dorsally to the mesenchyme associated with the foregut. Then, two coronal pleuropericardial folds appear at the lateral wall of the future intrathoracic pericardial cavity. They grow medially to fuse with each other and the septum transversum, forming the pericardial and pleural cavities. At this moment, the peritoneal and pleural cavities are still continuous with each other through two large dorsolateral openings; the pericardioperitoneal canals (Figure 6E). Finally, a pair of ventral growing transverse membranes, that already were present at the beginning of the fifth week, fuse with the posterior margin of the septum transversum. These pleuroperitoneal membranes finalize the complete sealing of the pericardioperitoneal canals by the end of the seventh week. 41 Interestingly, the left pericardioperitoneal canal is larger and closes later than the right one (Figure 6F).
The embryological development of the foregut (and its derivatives), the retroperitoneal space and the diaphragm.
Keeping in mind these critical steps of embryologic development, several hypotheses regarding the pathogenesis of retroperitoneal localized bronchogenic cysts were suggested.10,18,40,43 First, retroperitoneal bronchogenic cysts could be regarded upon as abnormally differentiated foregut duplication cysts originating intra-abdominal or retroperitoneal.10,39 Consequently, these lesions can be found in or near any organ derived from this primitive foregut (esophagus, stomach, superior half of the duodenum, liver, pancreas and gallbladder). 44 This hypothesis explains the occurrence of bronchogenic cysts in the region of the pancreas.10,15,17,19 liver9,22 and stomach. 8 However, even though duplications may occur anywhere along the embryonic gut tube, they are most commonly encountered at the level of the midgut. 43
A second, more plausible, hypothesis was proposed by Sumiyoshi et al. in 1985. 40 They postulated bronchogenic cysts as congenital anomalies resulting from abnormal budding of the respiratory diverticulum. When attachment to the primitive foregut persists, these lesions will develop in proximity to the tracheobronchial tree or oesophagus (the ventral, respectively dorsal components of the foregut). With closure of the parts forming the future diaphragm, these abnormal lung buds can be pinched off the developing tracheobronchial tree. Subsequently, they can get trapped in the diaphragm or, before complete fusion of the diaphragmatic components, migrate into the abdomen. The case report of W.M. Jo et al, describing a bronchogenic cyst extending from the pleural space into the retroperitoneum, provides an additional argument in favor of this hypothesis. 18 We strongly support the latter hypothesis, since it provides a rationale for the predominantly left sided location of retroperitoneal bronchogenic cysts. As already mentioned, the left pericardioperitoneal canal is larger and closes later than the right one. 41
Clinical aspects
Location
Bronchogenic cysts are usually benign, congenital anomalies that are most frequently encountered within the pulmonary parenchyma or in the posterior mediastinum.1,2 Bronchogenic cysts arising outside the thoracic cavity are rare. With respect to the subdiaphragmatic lesions, they are usually located retroperitoneal (behind the stomach) in a triangle defined by the midline, the splenic vein inferiorly and the diaphragm superiorly. 20 As reported in literature (Table 1), most retroperitoneal bronchogenic cysts are found near the left adrenal gland. The second most common location is the peripancreatic region.17,44 Similar to their mediastinal counterparts, retroperitoneal bronchogenic cysts usually are diagnosed incidentally. The exact prevalence is not known.
Signs and symptoms
Bronchogenic cysts are mostly asymptomatic. Due to continued epithelial secretion, these lesions have a tendency to become larger as the patients get older. 33 When they become symptomatic, it is usually due to secondary complications. Infection, perforation and hemorrhage are reported in literature.1,11,39 Due to normal growth or acute hemorrhage, bronchogenic cysts can compress adjacent structures. This may result in phaeochromocytoma-like symptoms due to pressure on the adjacent adrenal gland.20,28,35 Also more subtle symptoms, such as vague complaints of abdominal discomfort and early satiety, can be explained by this mechanism. 17
In 1941, Womack and Graham were the first to report metaplasia arising in the lining of congenital lung cysts. 45 Malignant degeneration in bronchogenic cysts is rare and most of the reported cases were located in the thoracic cavity. They include a bronchioalveolar carcinoma arising in a bronchogenic cyst of the lung,46,47 a malignant melanoma developing in a cutaneous bronchogenic cyst 6 and an adenocarcinoma originating in a bronchogenic cyst of the lung. 48 Only one case of a retroperitoneal bronchogenic cyst associated with the development of an adenocarcinoma has been reported. 49 However, since no ciliated cells were observed and ectodermal components were found, this case report did not fulfill anatomopathological criteria. Nevertheless, the authors still classified this lesion as a bronchogenic cyst. They suggested that malignant dysplastic changes resulted in the loss of cilia from epithelial cells and the observed bone (=ectodermal) tissue represented dystrophic calcification. The same pathological lack of clarity clouds other reported cases of malignant degeneration in bronchogenic cysts.1,47,50 Perhaps repetitive inflammatory episodes followed by scarring, contributes to both the loss of pathognomonic histological criteria and the increased risk for malignant degeneration.47,50 Also smoking and other habits could influence the development of malignancy. 47 Some authors even suggest there is an innate risk between lung maldevelopment and the occurrence of malignancy. 47
Differential diagnosis
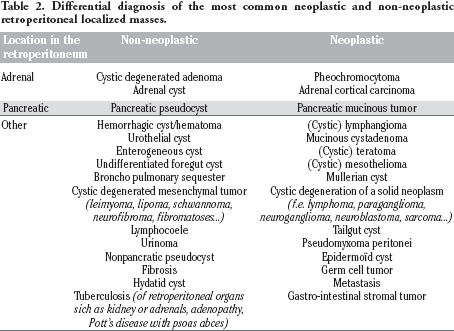
Retroperitoneal masses impose a broad differential diagnosis. Depending on their origin, the clinical implications and thus therapeutic strategies vary. In the past, Menke et al. stated that more than two-third of the retroperitoneal located tumors have malignant potential. 51 However, in that era only symptomatic lesions came to clinical attention. With more common use of radiological imaging, an increasing number of asymptomatic retroperitoneal lesions are incidentally discovered. 52 As a consequence, recent literature concerning retroperitoneal masses does not show a remarkable difference in prevalence between neoplastic and non-neoplastic lesions anymore.52,53 According to Tambo et al. 52 and Nakashima et al. 53 their occurrence even seems quite similar. The most important differential diagnoses are summed in Tables 2 and 3.
Differential diagnosis of the most common neoplastic and non-neoplastic retroperitoneal localized masses.
Differential diagnosis of retroperitoneal localized cystic masses lined by pseudostratified ciliated columnar epithelium.

Anatomopathological characteristics
Since bronchogenic cysts originate from the foregut, they consist of meso- and endoderm. The pathological criteria determining the exact diagnosis include the type of epithelial lining together with the structures composing the cystic wall. Infection or malignant degeneration could destroy or change some of these typical characteristics. 49
Bronchogenic cysts are mainly uni- or oligolocular cysts, lined by pseudostratified ciliated columnar epithelium. The latter typically rests on a fibrovascular connective tissue wall, containing at least one of the following: seromucous glands, smooth muscle cells or hyaline cartilage.1,20
The differential diagnosis of a retroperitoneal cyst lined by pseudostratified, ciliated, columnar epithelium includes other cysts of foregut origin, cysts of urogenital origin, a cystic teratoma or a bronchopulmonary sequestration20,23,29,32,42 (Table 3). As already mentioned, cysts originating from the primitive foregut can be classified into bronchogenic, enterogeneous and undifferentiated. Those cysts with ciliated or nonciliated epithelium containing two well-developed layers of smooth muscle without cartilage, can be classified as oesophageal cysts. Cysts with ciliated epithelium lacking other distinguishing features are called undifferentiated foregut cysts. When seromucous glands or cartilage are described, the diagnosis of an urothelial or mullerian cyst can be ruled out. A cystic teratoma is diagnosed when structures derived from all three germ layers are represented. Furthermore, a bronchogenic cyst has to be distinguished from other bronchopulmonary anomalies. The degree of development and location of these structures varies according to the stage of development in embryonic life during which they originated. 42 Since a bronchopulmonary sequestration includes mature lung parenchyma and pleural structures, it can be seen as created later during embryological development.
The fluid within the bronchogenic cysts consists of a mixture of water and proteinaceous mucus, with or without components due to previous hemorrhage or infection. This variability in cyst content provides a plausible explanation for the variability of attenuation on computed topographic (CT) scans and specific signal intensity characteristics on magnetic resonance imaging (MRI), as will be discussed in the next section.
Radiological features
On US these lesions show a variable internal echogenicity. Usually they appear anechoic with or without hyperechoic debris. 2 Since the retroperitoneal space is not readily accessible for US, this imaging modality never is the sole diagnostic tool of preference.
On CT examination, bronchogenic cysts typically appear as spherical lesions with well circumscribed smooth or lobulated borders. They are usually described as homogenous hypoattenuating (0–20HU, like water) lesions without enhancement after intravenous contrast administration. Hyperattenuation (coefficients up to 120HU) suggests hemorrhage or the presence of thick mucinous and proteinaceous secretions in the lesion.2,17,20 The latter lesions can be misdiagnosed as solid masses. In one case, the presence of a fluid-fluid level was described (high viscosity of the fluid at the bottom), indicating the cystic nature of the lesion. 15 Calcification of the cyst wall is possible. 2
On MRI a variable signal intensity has been described, which can be attributed to either the high protein content or the presence of methemoglobin due to hemorrhage.30,33,54 In general, simple fluid filled cysts are characterized by a very low signal intensity on T1-weighted images. The presence of protein and other paramagnetic substances in the fluid of bronchogenic cysts, generates a higher signal intensity. As a consequence, bronchogenic cysts usually show an intermediate to high signal intensity on T1-weighted images in combination with a markedly high signal intensity on T2-weighted images. Additionally, the signal intensity of the contents is not inverted in T1-weighted fat-suppressed images, excluding the diagnosis of a teratoma. Due to their contents, bronchogenic cysts may mimic the appearance of a solid mass on CT and T1-weighted MRI. However, the cystic nature will be characterized by a very high signal intensity on T2-weighted MRI.30,33,54
In Figures 1, 7 and 8 the MRI images of our case report are exhibited.
Magnetic resonance imaging of the retroperitoneal bronchogenic cyst. On the T2-weighted (HASTE TE=60 msec) images in the axial plane (A–D) the lesion can be seen adjacent to the left diaphragm (arrows). Furthermore, a small extension in the diaphragmatic pillar is demonstrated. The mixed signal intensity of the lesion is also demonstrated on T1-weighted images (TurboFLASH, E) as is on T2. This suggests a high protein content in some part of the lesion, besides fluid.
Magnetic resonance imaging-contrast enhancement image of the retroperitoneal bronchogenic cyst. A 3D T1 VIBE image in the axial plane. Only minimal contrast enhancement is seen after intravenous administration of gadolinium (Gd-DOTA, Dotarem® 15 mL). This enhancement occurs in the tiny septa, nodular solid components could not be demontrated in the lesion.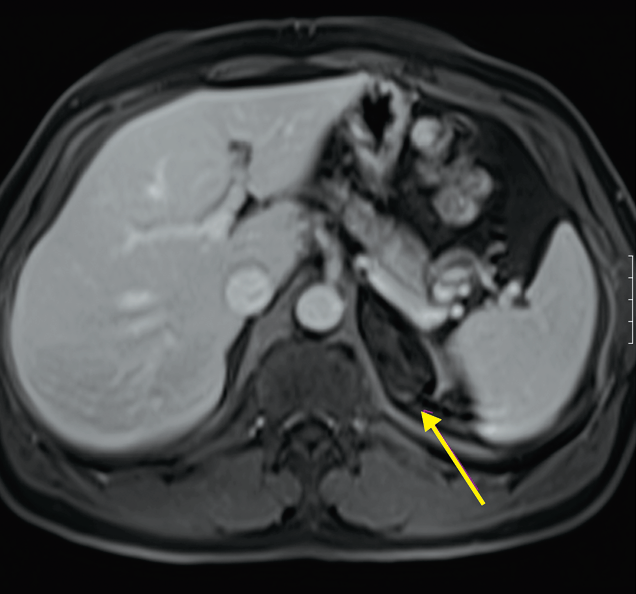
Biochemical features
Since most retroperitoneal bronchogenic cysts are located in close proximity to the left adrenal gland or pancreas, appropriate biochemical tests are essential in the diagnostic work-up. First of all, a distinction has to be made between both functional and non-functional adrenal masses. To exclude cushing's disease due to a cortisol-producing adrenal adenoma, careful clinical examination should be combined with the measurements of serum potassium, 24h urinary cortisol, serum cortisol after dexamethasone suppression test and basal serum ACTH levels. When clinical examination suggests a phaeochromocytoma, the following tests should be performed: urine levels of catecholamines (epinephrine, metanephrine, vanillylmandelic acid, dopamine) and plasma dosage of metanephrine and normetanephrine. Secondly, the pancreatic enzymes (serum amylase and lipase) have to be measured in the presence of peripancreatic lesions. A carcinoid can be excluded by means of urinary and plasma testing for serotonin or its metabolites (i.e. 5-Hydroxyindoleacetic acid or 5-HIAA) in urine. Finally, determining the following tumor markers can contribute to the diagnostic process of all retroperitoneal masses: cancer antigen 19-9 (CA 19-9), beta-human chorionic gonadotropin (β-HCG), alpha-feto-protein (AFP) and carcinoembryonic antigen (CEA).
Treatment
There are several arguments for removal of all retroperitoneal cystic or solid lesions. First, infection is an established complication of bronchogenic cysts. Since the complication rate of surgery with an infected cyst is high, removal of an uncomplicated cyst is warranted. 39 Secondly, given the broad differential diagnosis, it is impossible to establish an unequivocal diagnosis of a bronchogenic cyst preoperatively. Only anatomopathological examination can provide the definite diagnosis. Also, future malignant degeneration or the presence of a missed malignant tumor raises concerns. Failing to recognize and treat these pathological entities at the moment of diagnosis, can lead to disastrous consequences. For these reasons, early surgical resection of asymptomatic retroperitoneal cystic and solid masses is recommended in all good surgical candidates.
The surgical approach will be determined by the lesion's characteristics and location. Attachment to neighboring organs may necessitate their resection en bloc with these lesions. Patients should be informed about the potential need for resection of adjacent organs.
Several reports of laparoscopic excision of retroperitoneal bronchogenic cysts have appeared in recent literature.8,10,12,14,16,21,54,55 Since this approach uses smaller incisions, it has the potential to decrease hospital stay, postoperative complications and costs to the hospital and patient. Given the possibility of malignancy, the resected specimens should be removed within an endoscopic retrieval bag.
Retroperitoneoscopic excision could also be an ideal, less invasive approach. 26 It should be a safe and effective procedure, minimizing intraperitoneal adhesion formation and avoiding the need for visceral mobilization.24,56 In English literature we found only two publications describing three cases treated this way. Since these articles were published in 2002 and 2003, it raises the question why this technique has not yet become more popular.
Recent literature suggests retroperitoneoscopy to be a valid, less invasive surgical technique.13,24,56
Conclusions
Bronchogenic cysts are usually benign, asymptomatic cystic lesions. Most commonly they are encountered in the posterior mediastinum or in an intrapulmonary location. Keeping the embryological development in mind, the presence of bronchogenic cysts at more distant locations, such as the retroperitoneum, can be explained. In spite of the rarity of this pathologic entity, bronchogenic cysts should be considered in the differential diagnosis of retroperitoneal cystic and solid masses, especially when they are found in the left upper quadrant. Surgical resection of these lesions is recommended in order to alleviate any symptoms, to prevent complications (such as compression, infection, hemorrhage and future malignant transformation) and to establish a definite diagnosis. The combination of clinical, biochemical and radiological features sometimes helps in lesion characterization and choosing an adequate surgical approach. Only histology can provide the definite diagnosis.
A thorough search of literature, using strict anatomopathological criteria, revealed only 62 cases of retroperitoneal bronchogenic cysts reported worldwide, of which 46 appeared in the English-language literature. This article describes a case of a retroperitoneal bronchogenic cyst that presented as a non-functioning left adrenal mass. It intends to raise the index of suspicion to include this entity in the differential diagnosis of retroperitoneal cystic or solid masses. We provide recommendations concerning diagnosis and treatment of these lesions.
Footnotes
Acknowledgments:
we would like to thank Mr. Lieven Vanheessen and Mrs. Maud Dubois.