
Abstract
Papillary serous carcinoma of the uterine cervix (PSCC) is a very rare, recently described variant of cervical adenocarcinoma. This review, describes a case of stage IV PSCC whose main tumor existed in the uterine cervix and invaded one third of the inferior part of the anterior and posterior vaginal walls. Furthermore, it had metastasized from the para-aortic lymph nodes to bilateral neck lymph nodes. Immnoreactivity for CA125 was positive, whereas the staining for p53 and WT-1 were negative in both the original tumor and the metastatic lymph nodes. Six cycles of paclitaxel and carboplatin combination chemotherapy were administered and the PSCC dramatically decreased in size. The main tumor of the uterine cervix showed a complete response by magnetic resonance imaging (MRI), and on rebiopsy, more than 95% of the tumor cells in the cervix had microscopically disapperared. This is the first report of PSCC in which combination chemotherapy was used and showed a remarkable response.
Keywords
Introduction
Adenocarcinomas of the uterine cervix account for approximately 10–20% of invasive cervical carcinomas, and the endocervical types comprise approximately 70% of adenocarcinomas of the uterine cervix. 1 Papillary serous carcinoma of the cervix (PSCC) is an uncommon, recently described variant of cervical adenocarcinoma that is morphologically similar to papillary serous adenocarcinoma arising from the ovary, uterine endometrium, fallopian tube and peritoneum. In general, adenocarcinomas of the uterine cervix not only have poor chemosensitivity, but also poor radiosensitivity. This review describes an advanced PSCC case that exhibited a remarkable response to paclitaxel and carboplatin combination chemotherapy.
Case Report
A 56-year-old Japanese female, G4 P2, noticed a swollen lymph node in her right neck. She visited an otolaryngological clinic one month later. A lymph node biopsy was performed at this clinic. The pathologic diagnosis was PSC and was suspected to be metastatic adenocarcinoma. As she had also experienced a small amount of postmenopausal bleeding, she referred to the outpatient clinic (Department of Obstetrics and Gynecology) at our hospital. During the pelvic examination, a hard and swollen tumor of the uterine cervix was detected and had invaded the left and right parametrium to the pelvic wall as well as invasion to the inferior one third of the anterior and posterior vaginal walls. We performed a biopsy of the uterine tumor and obtained a diagnosis of PSCC microscopically (Figure 1). The tumor had a complex papillary pattern with epithelial stratification and tufting with the formation of cellular buds. In the nonpapillary parts, the tumor cells had a predominantly glandular growth pattern. The tumor cells had >10 mitotic figures per 10 high-power fields and scattered psammoma bodies.
The tumor had a complex papillary pattern with epithelial stratification and tufting with the formation of cellular buds. In the nonpapillary parts, the tumors cells had a predominantly glandular growth pattern and scattered psammoma bodies.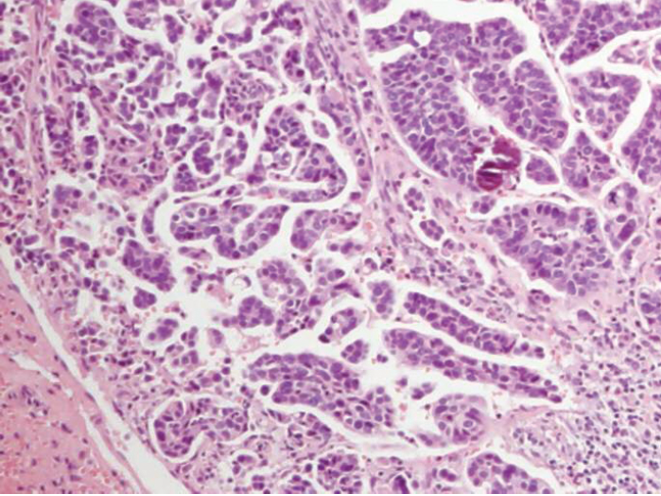
Immunoreactivity for CA125 was positive both in the uterine cervical tumor cells and the lymph node cells. On the other hand, immunoreactivity for p53 and Wilms’ tumor-1 (WT-1) was negative for both locations (Table 1). The pathologic characteristics of the right neck lymph node were consistent with those of the uterine cervix. We diagnosed the swollen neck lymph node as metastasis from the uterine cervical adenocarcinoma. The serum CA 125 level was elevated at 2480 U/mL (normal range <35 U/mL). Computed tomography (CT) scan revealed the swelling of multiple lymph nodes on bilateral sides of the patient's neck (Figure 2). Furthermore, it revealed the swelling of multiple lymph nodes in her mediastinum and para-aortic and pelvic lymph nodes. Lung and liver metastases were not seen. Magnetic resonance imaging (MRI) showed an enlarged uterine cervical mass and vaginal invasion to one third of the inferior parts (Figure 3). However, there was no evidence of a uterine endometrial tumor. The final clinical diagnosis was stage IVb PSCC.
Immunohistochemical expression of PSCC.

A computed tomography scan revealed the swelling of multiple lymph nodes on bilateral sides (arrows) of the patient's neck.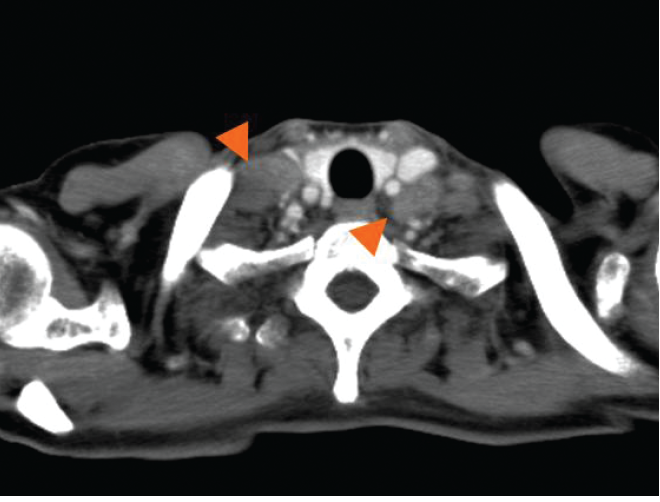
T2-weighted sagital magnetic resonance imaging showed an enlarged uterine cervical mass and vaginal invasion to one third of the inferior parts (arrows).
We selected a paclitaxel (175 mg/m2) and carboplatin (AUC 5) combination chemotherapy for the primary treatment. The patient received six courses of this chemotherapy after which her CA125 level fell to 45 U/mL. The tumor had been rapidly reduced in size by over 95%. CT scan showed an almost complete response based on the response evaluation criteria in solid tumors (RECIST). MRI also showed remarkable reduction of the uterine cervical tumor and vaginal masses (Figure 4). Re-biopsy of the uterine cervix demonstrated that nearly all of the carcinoma cells had disappeared, except for a small focus of atypical cells in the cervical stroma (>95% of the malignant cells had disapperared; Figure 5).
T2-weighted sagital magnetic resonance imaging showed an almost complete response based on the response evaluation criteria after the chemotherapy.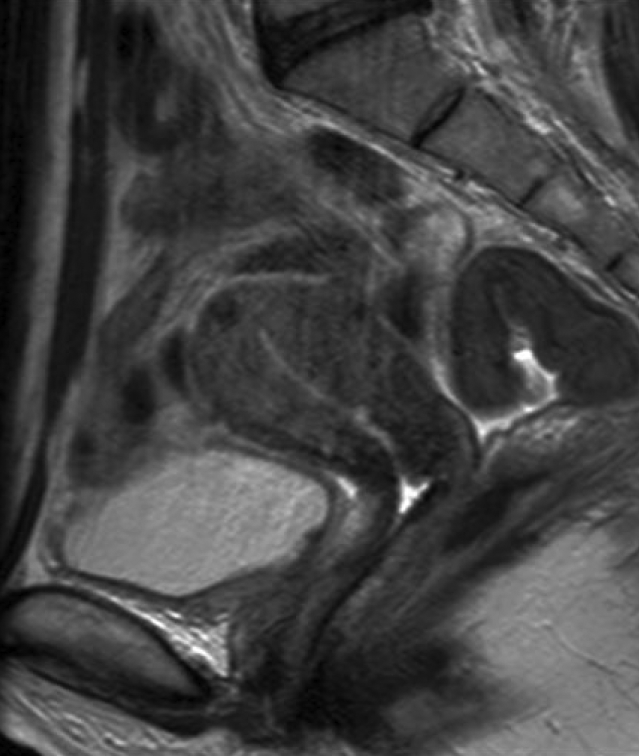
Almost all of the carcinoma cells had disappeared, except for a small focus of atypical cells in the cervical stroma microscopically.
We are planning a debulking surgery for this patient. If the tumor recurs, we will continue the chemotherapy.
Discussion
PSCC is a very rare specific subtype of endocervical adenocarcinomas. 1 To the best of our knowledge, only 45 cases of PSCC have been reported (Table 2).2–15 PSCC should be distinguished from other papillary carcinomas of the cervix, such as low-grade papillary villoglandular adenocarcinoma, a variant of endocrevical adenocarcinoma with a good prognosis. In the 45 previously reported cases of PSCC, some cases were actually villoglandular adenocarcinomas or mixed types tumors. 9 With regard to our case, the tumors were composed of papillary tufts and complex papillae lined by cells with pleomorphic, high-grade nuclei, numerous mitotic bodies, and psammmoma bodies, which were typical of PSCC.
Other papillary serous carcinomas occur from the ovary, uterine endometrium, fallopian tube and peritoneum. In our case, the main tumor existed in the uterine cervix, but the endometrium was thin. We did not find ovarian masses, omental cakes or tubal masses. Using MRI and CT scans, we diagnosed this tumor to have originated from the uterine cervix. By an immunohistochemical analysis, we examined the expression of CA125, p53 and WT-1 in the tumor. Our PSCCs were immunopositive for CA125, but negative for p53 and WT-1. Zhou et al reported that 9 of their 12 (75%) PSCCs were CA125 immunopositive. 9 The p53 immunopositivity ranged from 42–90% in the previous reports.9,13 Recently, immnunopositivity for p53 has been reported to be an early event in PSCC, because p53 expression was detected diffusely in PSCC in situ. 15 It was similar to papillary serous carcinomas of the endometrium (PSCE) 16 and serous carcinoma of the ovary. 17 WT-1 immmunostaining has been thought to be useful in distinguishing serous carcinomas of the ovary, which are mostly immunopositive for WT-1, from PSCEs, which are generally most immunonegative for WT-1. 13 Our PSCC was also immunonegative for WT-1. These findings suggest that our case of papillary serous carcinomas arose from the uterine cervix, and was not a metastasis from the ovary.
Number of patients with PSCC in previous reports.

With regard to the treatment of PSCC, primary surgical therapy has been thought to be preferable to primary radiotherapy in the early stage. 9 Hysterectomy, radical hysterectomy and trachelectomy have been used as the primary surgery, followed by postoperative radiotherapy.9,13 However, PSCCs are aggressive neoplasms and usually found with lymph node metastases. Occasionally, PSCCs are found at advanced stages, such as stage III or IV.
To our knowledge, there were no reports of the effect of primary chemotherapy against advanced PSCC cases. Therefore, there was no evidence of the chemosensitivity of the disease. Our PSCC case was diagnosed at stage IVb. Therefore, we could not perform primary surgery, and elected to administer a combination chemotherapy using paclitaxel and carboplatin. We selected this combined regimen as the first line chemotherapy, because it is currently the recommended combination used for the treatment of ovarian cancers18,19 and is known to have good efficacy against serous carcinoma of the ovary. 20 The recommended dose for this combination regimen is thought to be paclitaxel 175 mg/m2 plus carboplatin AUC 6 (maximum dose, 800 mg/body). 21 Usually the general treatment for ovarian cancer should be repeated for six to eight courses. In this case, we obtained an excellent response to a combination therapy with paclitaxel and carboplatin. Our PSCC had aggressive activity (tumor cells had >10 mitotic figures per 10 high-power fields) and good chmosensitivities to paclitaxel and carboplatin just like serous carcinoma of the ovary. Induction of tumor cell death by chemotherapeutic agents often occurs in a cell cycle-dependent manner. It has also been observed that several regulatory proteins involved in tumor chemosensitivity and apoptosis are expressed periodically during the cell cycle progression. However, the nature of cancer cellular chemosensitivity and mechanisms of action of anti-cancer drugs in different phases of the cell cycle still remain unknown. In addition, clinical analysis of molecular biomarkers that predict responses to chemotherapeutic agents in uterine cervical carcinomas has not been carried out. When an advanced case of unresectable PSCC is encountered, however, we recommend the use of primary paclitaxel and carboplatin combination chemotherapy, and also believe that this regimen can be used as an effective neoadjuvant chemotherapy to be performed prior to radical surgery.