
Abstract
Primary gastric chorioadenocarcinoma (PGC) is an exceedingly rare neoplasm which is often misdiagnosed as gastric adenocarcinoma at presentation. A markedly elevated serum beta human chorionic gonadotrophin (Beta HCG) level is a characteristic feature of this tumor. A 44 year old white male presented with generalized abdominal pain and fullness, tarry black stools and weight loss of 3 months duration. Medical work-up including imaging with CT scans revealed the presence of a gastric mass and multiple liver metastases. Tumor markers were significant for a Beta human chorionic gonadotrophin (Beta HCG) of 23717.5 MIU/ML. Scrotal ultrasound did not show the presence of a testicular mass. Upper GI endoscopy with biopsy was positive for a poorly differentiated adenocarcinoma with Beta HCG staining on immunohistochemistry. The patient was diagnosed with metastatic PGC. He received four cycles of chemotherapy with Bleomycin, Etoposide and Cisplatinum. At the end of the fourth cycle, Beta HCG was 23 MIU/ML. CT scan for restaging, however showed an increase in the size of the metastatic lesions. The patient subsequently became profoundly pancytopenic, developed disseminated intravascular coagulation (DIC) and expired 12 months after initial presentation. PGC genetically and morphologically represents an adenocarcinoma and a choriocarcinoma. The significance of an elevated serum Beta HCG is controversial and it may have a role in evaluating response to treatment and tumor recurrence. Curative resection, appropriate chemotherapy and the absence of metastatic lesions is associated with improved survival. Hence, a high index of suspicion must be maintained to diagnose this tumor correctly at presentation and tailor therapy accordingly.
Introduction
Primary gastric chorioadenocarcinoma (PGC) is an exceedingly rare neoplasm with approximately 30 PGC cases reported to date in the English-language medical literature. 1 PGC accounts for less than 1% of all gastric malignancies. 2 As the name suggests, the tumor consists of gastric adenocarcinoma cells admixed with cytotrophoblast and syncytiotrophoblast cells that constitute the choriocarcinomatous component. The first clue to diagnosis is often a markedly elevated serum beta human chorionic gonadotrophin (Beta HCG) level.3–5 We describe an interesting case of PGC that was treated at our institution, with an initial dramatic response to chemotherapy and gradual progression thereafter.
History and presentation
A 44 year old white male with no significant past medical history presented with generalized abdominal pain and tarry black stools of 3 months duration. He also complained of increased abdominal girth, abdominal fullness, night sweats, weight loss and fever of 2 months duration. Physical exam was significant for a distended abdomen which was tender to palpation in the right upper quadrant. Computerized tomography (CT) of the thorax (Figure 1), abdomen and pelvis revealed mediastinal lymphadenopathy, bilateral pulmonary nodules, and an abnormally increased thickness of the wall of the body of the stomach. An 8.0×5.7 cm soft tissue mass adjacent to the lesser curvature of the stomach which was extending caudally to the level of the pancreas (Figure 2).
Computerezed tomography scan of the abdomen with contrast. Increased thickness of the wall of the body of the stomach and multiple metastatic lesions in the right and left lobe of the liver.
Computerezed tomography scan of the abdomen with contrast. An 8.0 × 5.7 cm soft tissue mass adjacent to the lesser curvature of the stomach extending caudally to the level of the pancreas. Multiple metastatic lesions in the right and left lobe of the liver.
There were a few slightly enlarged lymph nodes adjacent to the pancreatic head and in the porta hepatis, multiple mass lesions in the right and the left lobe of the liver and moderate ascites. Tumor markers were significant for a markedly elevated Beta HCG of 23717.5 MIU/ML and elevated alpha fetoprotein (AFP) of 21.07 NG/ML. Scrotal ultrasound did not reveal the presence of a testicular mass. The patient underwent an upper GI endoscopy with biopsy which revealed a malignant appearing ulcerated mass involving the whole gastric cardia. Biopsy of the mass was consistent with a poorly differentiated carcinoma with features of a chorioadenocarcinoma. Immunohistochemical staining was strongly positive for Beta HCG in a large component of the biopsied mass (Figure 3, 4). CT guided FNA and core biopsy of the liver showed pleomorphic cells with a high mitotic rate and large irregular nuclei consistent with choriocarcinoma (Figure 5). In the absence of a primary testicular mass, the patient was diagnosed with a primary gastric chorioadenocarcinoma with liver, lung and mediastinal metastasis.
Immunohistochemical stain. Gastric biopsy specimen with intestinaltype adenocarcinoma composed of columnar gland forming cells interspersed with cytotrophoblast and syncytiotrophoblast cells staining positve for Beta HCG on IHC (Immunohistochemistry).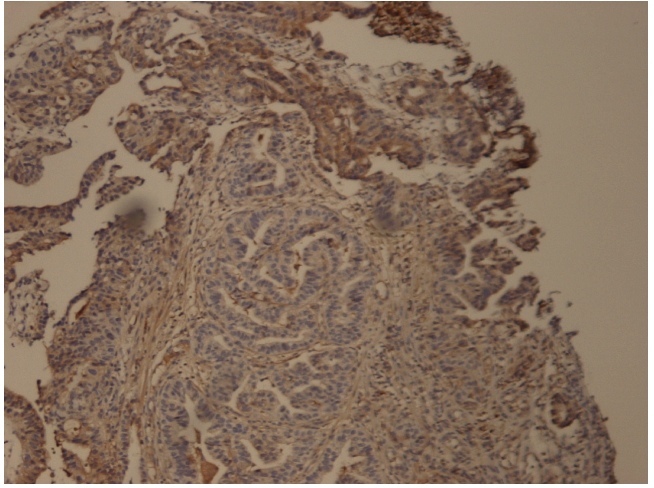
Immunohistochemical stain. Gastric biopsy specimen from the patient with Beta HCG staining (brown) on Immunohistochemistry.
Hematoxylin & Eosin stain. The tumor appears to be pleomorphic with a high mitotic rate. There are several large cells with large irregular nuclei.
As the patient had extensive metastatic disease on presentation, a surgical procedure to decrease tumor burden would have involved high morbidity. Hence, chemotherapy with bleomycin, etoposide and cisplatin (BEP) was started, to decrease the tumor burden. Chemotherapy was interrupted, initially due to tumor lysis syndrome and acute tubular necrosis causing acute renal failure secondary to cisplatin which subsequently resolved, and then due to recurrent Clostridium difficile infections.
At the end of 4 cycles of chemotherapy with BEP, the tumor markers showed dramatic improvement, with Beta HCG down to 23 MIU/ML from 23,717 MIU/ML at initial presentation. A repeat CT scan for restaging showed decrease in size of the gastric mass and liver lesions but increased right sided mediastinal lymphadenopathy. Despite the initial dramatic response of the tumor markers to chemotherapy, the metastatic lesions in the liver and ascites continues to progress. The patient eventually had bone marrow involvement with tumor and became profoundly pancytopenic, necessitating multiple transfusions. He ultimately developed disseminated intravascular coagulation (DIC) and passed away 12 months from initial presentation and diagnosis.
Discussion
The genesis of PGC, a rare and interesting tumor, is still a subject of controversy. Scientific opinion appears to support the dedifferentiation theory first proposed by Pick in 1926. 1 Liu et al. 6 reported the first interphase cytogenetics study of PGC, the results of which support the theory that gastric chorioadenocarcinoma arises from alternate differentiation pathways of adenocarcinoma. Except for the gain of chromosome 12, which is known to be uncommon in gastric adenocarcinoma but frequently associated with choriocarcinoma, the remaining genomic imbalances(gains of function mutations in 2q, 7pq, 8pq, 13q, 17q, 18q, 20pq and deletions in 17p) 7 were among the most common comparative genomic hybridization findings reported in gastric adenocarcinoma. Several other studies have indicated that the pathogenesis of PGC can be explained as the dedifferentiation of malignant adenocarcinoma tissue to the level of the embryonal ectoderm, retaining the ability to form trophoblasts. 4 Hence due to the coexistence of adenocarcinoma and choriocarcinoma, PGC is often misdiagnosed as an adenocarcinoma at presentation. Only 8% of the PGC cases in a pooled analysis of 53 cases were correctly diagnosed as choriocarcinoma by biopsy. 1 On gross appearance, gastric choriocarcinomas are exophytic. They are generally more beefy red and hemorrhagic than typical gastric adenocarcinomas, given their striking vascularity. 3 Histologically, there is a combination of malignant cytotrophoblast and syncytiotrophoblast, generally admixed with areas of typical glandular differentiation. 3
The syncytiotrophoblast cells stain positive for Beta HCG on immunohistochemistry. 8 Most cases of PGC described in the literature have been accompanied by elevated Beta HCG at presentation.3–5 This is responsible for the morning sickness like symptoms in women and gynecomastia in men presenting with this tumor. 3 The presence of the beta-HCG-positive cells in the gastric carcinomas suggested no appreciable prognostic significance, even quantitatively. 8 However, the significance of an elevated serum Beta-HCG in gastric choriocarcinoma is still controversial. While some studies suggest that it is associated with a shortened survival and poorer prognosis, others suggest that it has no prognostic significance. 5 Nonetheless, monitoring serial levels of Beta HCG post-operatively or post-chemotherapy may be a useful marker for evaluating response to treatment and tumor recurrence.
The major entity in the differential diagnosis of PGC is metastatic trophoblastic tumor from other sites, particularly gonadal or gestational primaries in women of reproductive age. 3 Although the number of well-documented cases of gastric choriocarcinomas reported to date is small, it appears that these tumors behave more like gestational or germ cell choriocarcinomas with rapid and extensive hematogenous dissemination as opposed to the preferred lymphatic spread of adenocarcinomas. Metastatic disease frequently contains pure choriocarcinoma, although mixed chorioadenocarcinoma metastases have also been seen. 5
This may explain the initial response of the metastatic lesions to platinum based chemotherapy and the initial large decrease in Beta HCG in our patient whose metastatic lesions on liver biopsy had pathology consistent with choriocarcinoma.
Gastrectomy with lymph node dissection followed by postoperative chemotherapy is the treatment of choice in patients with a limited tumor burden. 3 This treatment guideline is more by consensus than evidence-based practice. Kobayashi et al. 1 reported that the presence of residual tumor and synchronous liver metastasis and the absence of chemotherapy were significantly associated with an increased hazard rate (HR) of short overall survival (OS). They suggest that a palliative gastrectomy should never be performed in patients with synchronous liver metastasis, as it is likely to contribute to early post-procedure mortality. One may hence argue that it is better to first treat patients with synchronous metastasis at presentation with chemotherapy and monitor them with serial tumor marker levels and serial imaging for response prior to considering an operative procedure. Noguchi et al. 9 have reported a good treatment response with the combination therapy of 5-flurouracil and cisplatin.
Conclusion
PGC is a rare malignancy which has been identified and reported from time to time from different parts of the world, most notably Japan and the United States. A high index of suspicion must be entertained to diagnose this tumor, as it is commonly misdiagnosed on biopsy. Elevate Beta HCG is a clue obtained at presentation. Most of the tumors are at an advanced stage at presentation and have a poor prognosis. PGC is not as chemotherapy sensitive as pure choriocarcinomas. Despite having a pooled analysis of 53 cases reported, there are no clear guidelines yet about the appropriate treatment protocol for this tumor.
A larger sample size and more data analysis will be required to address the issue of finding an appropriate chemotherapy regimen.