
Abstract
Sarcomas are a rare occurrence accounting for roughly 1% of all cancer cases reported. Of these, 9–18% will be identified as liposarcoma. Overall, only 4–9% of all liposarcomas occur in the head and neck region. As such, it is a rare event to see a primary liposarcoma of the aerodigestive tract. These tumors are typically misdiagnosed secondary to their indolent, asymptomatic course and similarities in appearance to other benign lesions. An understanding of these lesions will help clinicians appropriately manage their patients. We present a case of a 60-year male with a primary supraglottic myxoid liposarcoma, and provide relevant information about liposarcomas.
Keywords
Introduction
Sarcomas are malignant neoplasms arising from connective tissue. They represent roughly 1% of all cancer cases reported. One subtype of sarcoma is liposarcoma. This type of sarcoma represents anywhere from 9–18% of all reported sarcoma cases, with only 4–9% occurring in the head and neck region.1,2 Although more common in other areas, it is rarely found in the aerodigestive tract.2–8 We present a case of a primary liposarcoma of the supraglottic larynx in an adult male.
Case Report
A 60-year old male presented to our clinic with complaints of progressive dysphagia to solids and liquids along with hoarseness and occasional choking episodes. He had been initially evaluated by a gastroenterologist who performed an esophagram that showed fullness in the hypopharynx but normal motility and no mucosal irregularities. Upon further questioning, the patient revealed having undergone removal of a benign fibrolipoma from his cervical esophagus in 2002. He had a history of smoking but denied alcohol or drug use. Upon examination, he was found to have a polypoid lesion involving his left arytenoid. His true vocal cords were mobile, and the remainder of the head and neck examination was unremarkable. The patient was taken to the operating room for biopsy. Pathological examination revealed a benign fibroepithelial polyp. Two months later, the patient presented with worsening dysphagia, hoarseness, dyspnea, and inspiratory stridor. Upon fiberoptic laryngoscopy, he was found to have multiple polypoid lesions involving the left arytenoid, left aryepiglottic fold, and post-cricoid region (Figure 1).
Image obtained by flexible laryngoscopy showing the multiple supraglottic polypoid lesions (arrows) and thickening of the left aryepiglottic fold (arrowhead).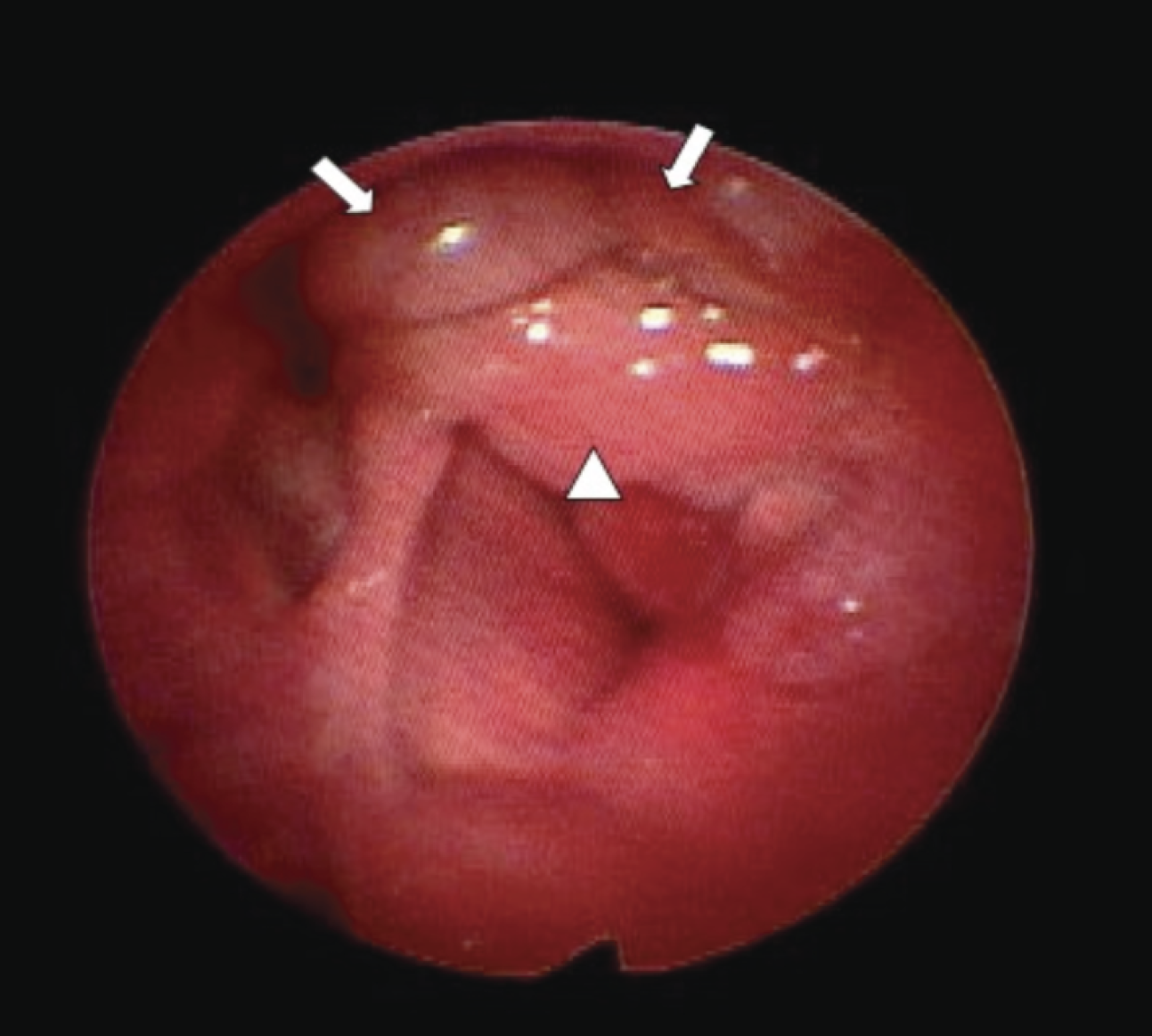
The lesions were now causing significant airway obstruction, and so the patient underwent tracheostomy with further biopsies. Although pathological evaluation revealed benign squamous tissue with chronic inflammation, a subsequent CT scan was of greater concern. This revealed a 3.5×3.3×3.2 cm heterogeneous laryngeal mass that occluded the airway and invaded through the thyroid cartilage (Figure 2).
Axial CT images with contrast showing the laryngeal lesion invading and destroying the thyroid cartilage (arrows) while also significantly narrowing the patient's airway (arrowheads).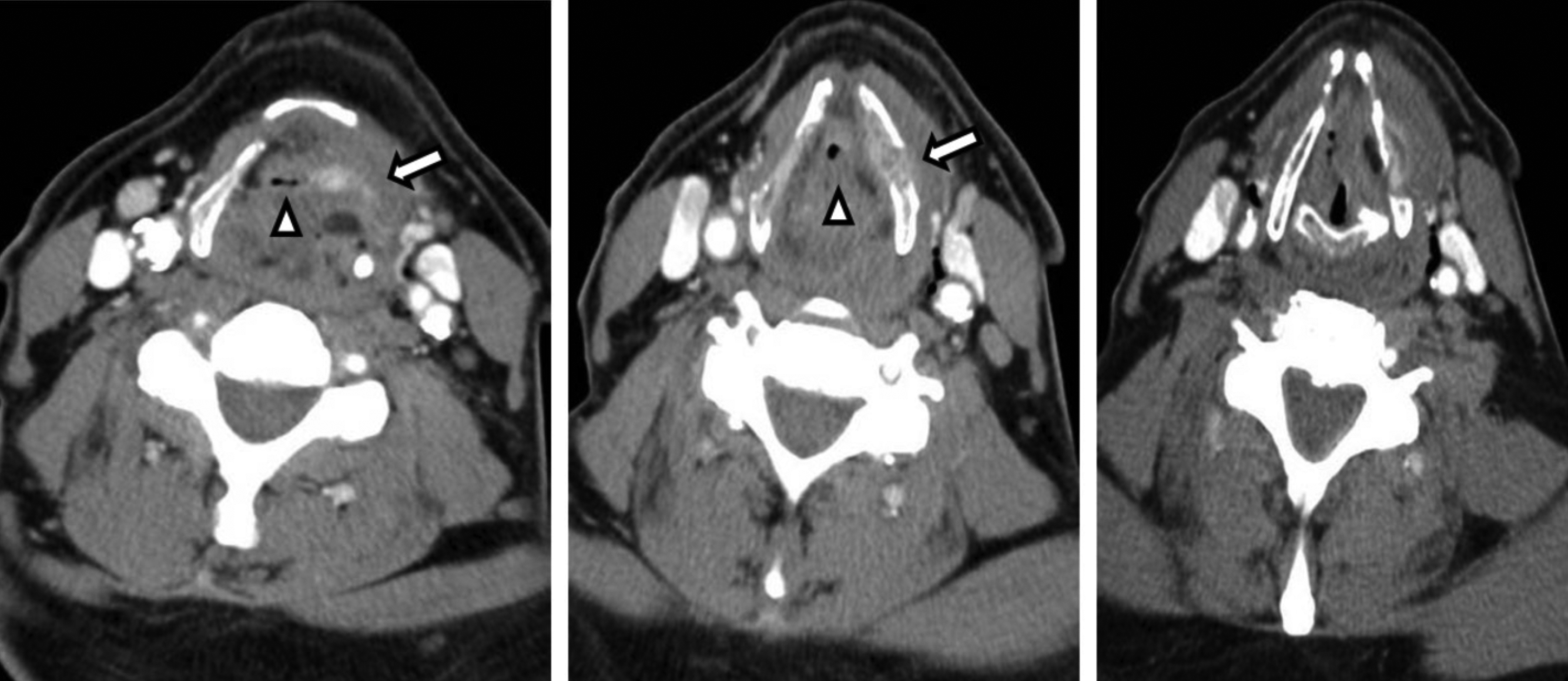
Therefore, the patient was taken back to the operating room, and larger biopsies were obtained using a CO2 laser, which demonstrated a liposarcoma. The patient subsequently underwent a total laryngectomy, partial pharyngectomy and reconstruction with an anterolateral thigh free flap. Gross examination of the laryngectomy specimen revealed a submucosal, yellowish-white polypoid mass measuring 6.2×6×2.5 cm arising from the left supraglottic region and partially obliterating the glottis. Microscopic examination showed mature adipose tissue with occasional lipoblasts as well as focal areas of myxoid differentiation containing atypical spindle cells with large, hyperchromatic nuclei, consistent with a well-differentiated myxoid liposarcoma (Figure 3).
(Top panel) Submucosal polypoid liposarcoma (arrows) arising from the left supraglottic region. (Bottom left) Well-differentiated liposarcoma with an area of myxoid differentiation. (Bottom right) (H&E, ×40). (Bottom middle) Myxoid differentiation (H&E, ×200). (Bottom right) Lipoblasts (arrows) with vacuolated cytoplasm and atypical nuclei (H&E, ×600).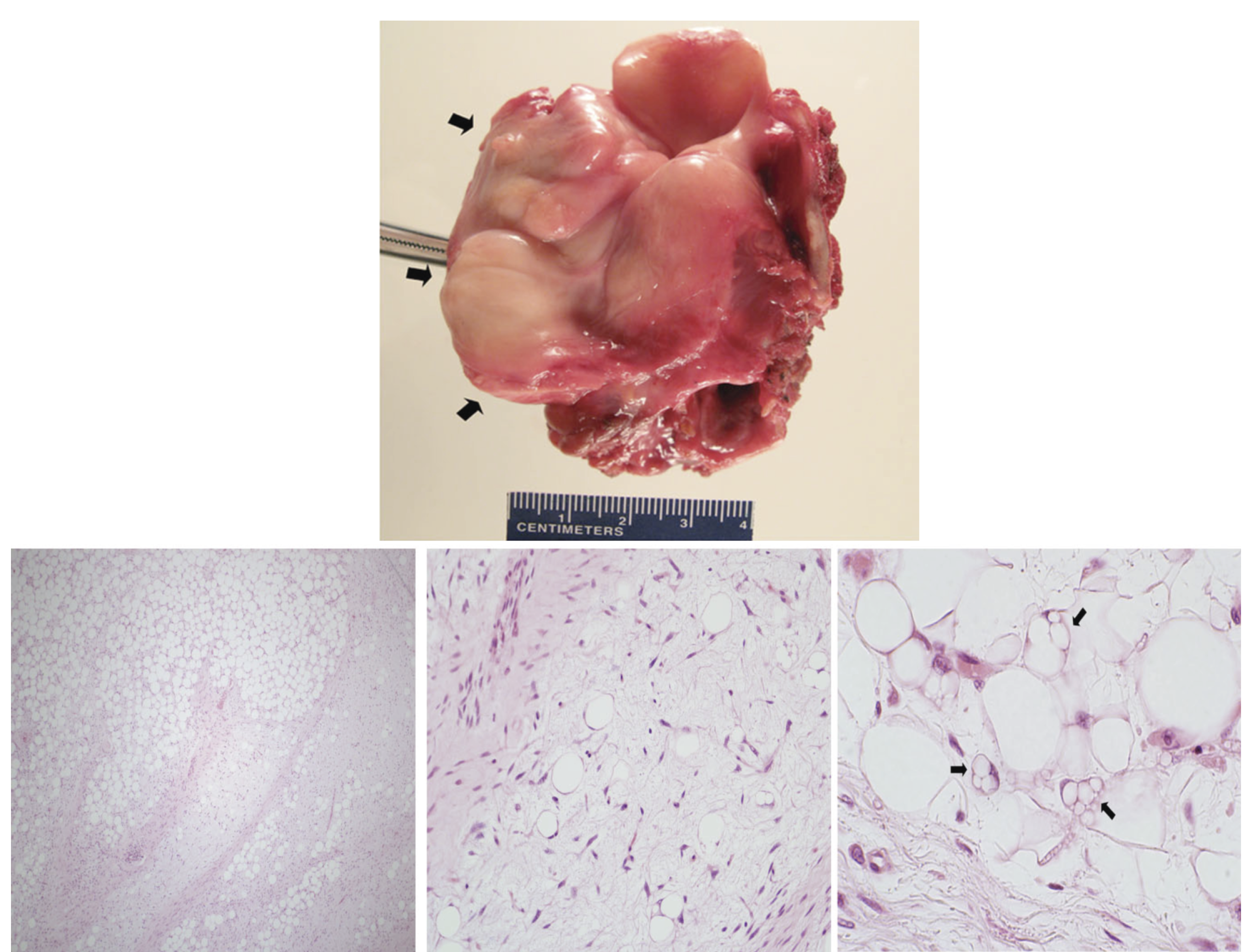
The patient has remained free of neoplastic recurrence for over a year and a half.
Discussion
A liposarcoma is a malignant mesenchymal neoplasm arising from deep-seated adipose tissue. Although rare, there have been reports of these neoplasms arising from pre-existing lipomas. 9 Liposarcomas are the second most common soft tissue sarcoma. They represent roughly 9–18% of all sarcomas, and tend to have a high predilection for the extremities and retroperitoneum.1,2 Overall, only 4–9% of all liposarcomas occur in the head and neck region. 2 Roughly 80% of these neoplasms occur in adults with a peak incidence around 40–60 years of age. 10 Their occurrence in children is very rare accounting for less than 5% of all soft tissue sarcoma cases in children.9,11
Liposarcomas are classified by their histopathological appearance. There are five recognized subtypes: well-differentiated, myxoid, round-cell, dedifferentiated, and pleomorphic. The myxoid subtype is the most common subtype, representing anywhere from 45–55% of cases. These tumors are considered low to intermediate grade. The well-differentiated subtype is the second most common subtype and represents 30–40% of cases. It is the lowest grade of all subtypes, and as such, tends to carry a better prognosis. The round-cell subtype is considered the high-grade counterpart of the myxoid subtype and typically represents 15% of all cases of liposarcomas. The dedifferentiated subtype is believed to arise from long standing or recurrent well-differentiated tumors. Depending on the amount of dedifferentiation, these can be intermediate or high grade. The pleomorphic subtype is the highest grade subtype, and caries the worst prognosis. Fortunately, this subtype is rare, accounting for only 5% of all liposarcoma cases.1,2,9–11 The pathogenesis behind these neoplasms is believed to involve various chromosomal abnormalities. The well-differentiated subtype is known to be associated with abnormalities of 1q and 12q13–15, while the myxoid and round-cell subtypes tend to have translocations. The most common of these translocations is the t(12;16)(q13;p11.2) translocation. This involves the fusion of the
The diagnosis of a liposarcoma is typically delayed secondary to its indolent, asymptomatic course. Upon gross inspection, these tumors appear very similar to those of lipomas. However, there are details that help to differentiate the two. Liposarcomas tend to be more fixed to the underlying tissue, less compressible, and firmer to palpation. They also tend to be less lobulated and less yellow in color when compared to lipomas.1,9,11 There are multiple imagining modalities available to aid the clinician in diagnosing liposarcomas. Of these, the most commonly utilized are the MRI and CT scans. The MRI is probably the most useful since it may reveal characteristics of the tumor that are suggestive of malignancy. On MRI, liposarcomas appear well-circumscribed and lobulated with thick, fibrous septae and nodularity. In addition to these findings, the presence of hemorrhage, edema, and areas of necrosis may also be noted, which may hint at malignancy. The level of enhancement can also be utilized in assessing these tumors. Low-grade liposarcomas tend to exhibit faint enhancement following contrast while their high-grade counterparts typically enhance very well with contrast. The amount of heterogeneity is also important as it can aid in determining the grade of the tumor. Well-differentiated liposarcomas typically appear homogeneous while myxoid types exhibit slight heterogeneity. The dedifferentiated, round cell, and pleomorphic types tend to exhibit moderate to marked heterogeneity.1,9,11 The gold standard in diagnosing a liposarcoma remains the biopsy. This can be done through fine needle aspiration and incisional or excisional biopsy. Some recommend avoidance of excisional biopsy in suspected cases of liposarcoma as it may negatively affect treatment planning.1,9–11 While each subtype has its own pathological characteristics, the key to the diagnosis is the presence of the lipoblast.5,12 Our patient's type is a myxoid liposarcoma. These tumors are characterized by three main features. The first is the presence of multiple lipoblasts in various stages of development. The second feature is the presence of a delicate plexiform capillary network. Finally, the stromal matrix is composed of hyaluronidase-sensitive acid mucopolysaccharides. The least cellular forms are considered lower grade tumors, and typically contain more spindle-shaped cells. The high cellular forms are considered high grade, and typically exhibit an abundance of round cells.1,9,11,13
The mainstay of treatment for liposarcomas is surgical excision. This is performed through wide or radical excision of the tumor. Since a positive margin is strongly correlated with tumor recurrence, it is extremely important to obtain tumor free margins. The rate of recurrence has been reported to increase from 17% to 80% with incomplete excision. There is no consensus on the amount of free margin required, but some surgeons recommend obtaining at least two centimeters of free margin. Elective neck dissection is not recommended as regional nodal metastasis is extremely rare.1,10–14
The use of adjunctive treatments in the overall treatment of liposarcoma remains controversial. The most common adjunctive treatment used is radiotherapy. A number of studies have shown improved local control and survival rates when radiotherapy is combined with surgery. Spiro
Conclusions
Liposarcoma of the head and neck remains a rare occurrence, especially as a primary tumor of the aerodigestive tract. These tumors are typically misdiagnosed secondary to their indolent course and similarities in appearance to more commonly encountered benign lesions. Once indentified, these tumors are best treated with wide surgical excision with a consideration for adjuvant radiotherapy. The use of chemotherapy remains controversial, and as such, further study is required to determine its effectiveness in the treatment of liposarcomas.