
Abstract
We describe here a case of pure gastric yolk sac tumor (YST). A 62-year-old patient underwent gastrectomy with D2 dissection. The histological report confirmed the diagnosis of YST and that two of the 14 regional lymph nodes removed were metastatic. Three courses of PEB regimen chemotherapy were delivered subsequently. Three months later the patient experienced dysphagia from stenosis of the anastomosis and a computerized tomography scan showed tumor recurrence with peritoneal nodules; the patient died one year after surgery. The origin of gastric YST is unclear but involvement of migrating germ cells during embryonic development or multipotential neoplastic protoepithelial cells of the gastric mucosa have been suggested. Generally the prognosis of gastric YST is poor and the standard therapeutic approach beyond surgery is still uncertain.
Case Report
A 62-year-old man was admitted to our hospital with a medical history of gastroesophageal reflux and dyspepsia lasting for three years, and a complaint a few days before admission of gastric pain associated with severe asthenia. Weight loss and severe anemia (6.5 g/dL) were also recorded.
Gastroscopy examination revealed a large ulcerated tumor located in the antrum, whereas chest and abdominopelvic computerized tomography (CT) scans did not demonstrate distant metastases. As a preoperative histological diagnosis of adenocarcinoma was rendered on small tissue biopsies taken during endoscopic evaluation, the patient underwent total gastrectomy with D2 dissection and omentectomy followed by digiunostomy.
The tumor, with a maximum diameter of 7 cm, was composed microscopically of neoplastic cells with pale eosinophilic to water-clear cytoplasm including some hyaline droplets and with round to oval vesicular nuclei and variably sized nucleoli. Tumor cells were arranged into solid and papillary or pseudopapillary structures (Figure 1A and B) with several glomeruloid aggregates resembling Schiller-Duval bodies (Figure 1B). These cells showed immunoreactivity for cytokeratins (Figure 1C) and α-fetoprotein (Figure 1D) but not for chromogranin A, cytokeratins 7 and 20, β-HCG, CDX2, placental alkaline phosphatase, and CD30. Immunostains for CEA and EMA were completely negative as one would expect for a case of pure gastric yolk sac tumor (YST). In order to exclude foci of conventional gastric adenocarcinoma or another germ cell tumor, we processed a paraffin block for every centimeter of gross tumor size, cutting and examining each block at three different levels: no other components were found, which reinforced the final diagnosis of YST. The surgical margins were free of disease but two out of the 14 regional lymph nodes removed were metastatic. All these morphological and immunohistochemical findings were consistent with the diagnosis of YST. Postoperatively α-fetoprotein was 4.8 ng/mL (normal range: 0–10 ng/mL). A subsequent objective examination of the patient did not reveal any lesion at testicular sites. The patient underwent chemotherapy with three courses of PEB regimen (cisplatin 100 mg/mq, day 1; etoposide 100 mg/mq, days 1–3; bleomycin 30 mg, days 2, 9, 16; but omitting bleomycin on days 2 and 9 after the first cycle). In addition, support with granulocyte stimulating factor was needed because of hematological toxicity. Three months after the end of chemotherapy the patient experienced dysphagia from stenosis of the anastomosis and an abdominopelvic CT scan showed tumor recurrence with peritoneal nodules and ascites. The α-fetoprotein was >50 ng/mL. As the patient deteriorated rapidly with systemic fever and abdominal pain, parenteral nutrition was started without administering further antitumor treatments. Death occurred one year after surgery.
Histological features of a gastric yolk sac tumor. (A) Tumor cells, with pale eosinophilic cytoplasm and vesicular nuclei, appear to be arranged into solid and papillary or pseudopapillary structures. (B) Several glomeruloid aggregates of the neoplastic cells resembling Schiller-Duval bodies are evident. The tumor cells showed immunoreactivity for cytokeratins (C) and for α-fetoprotein (D).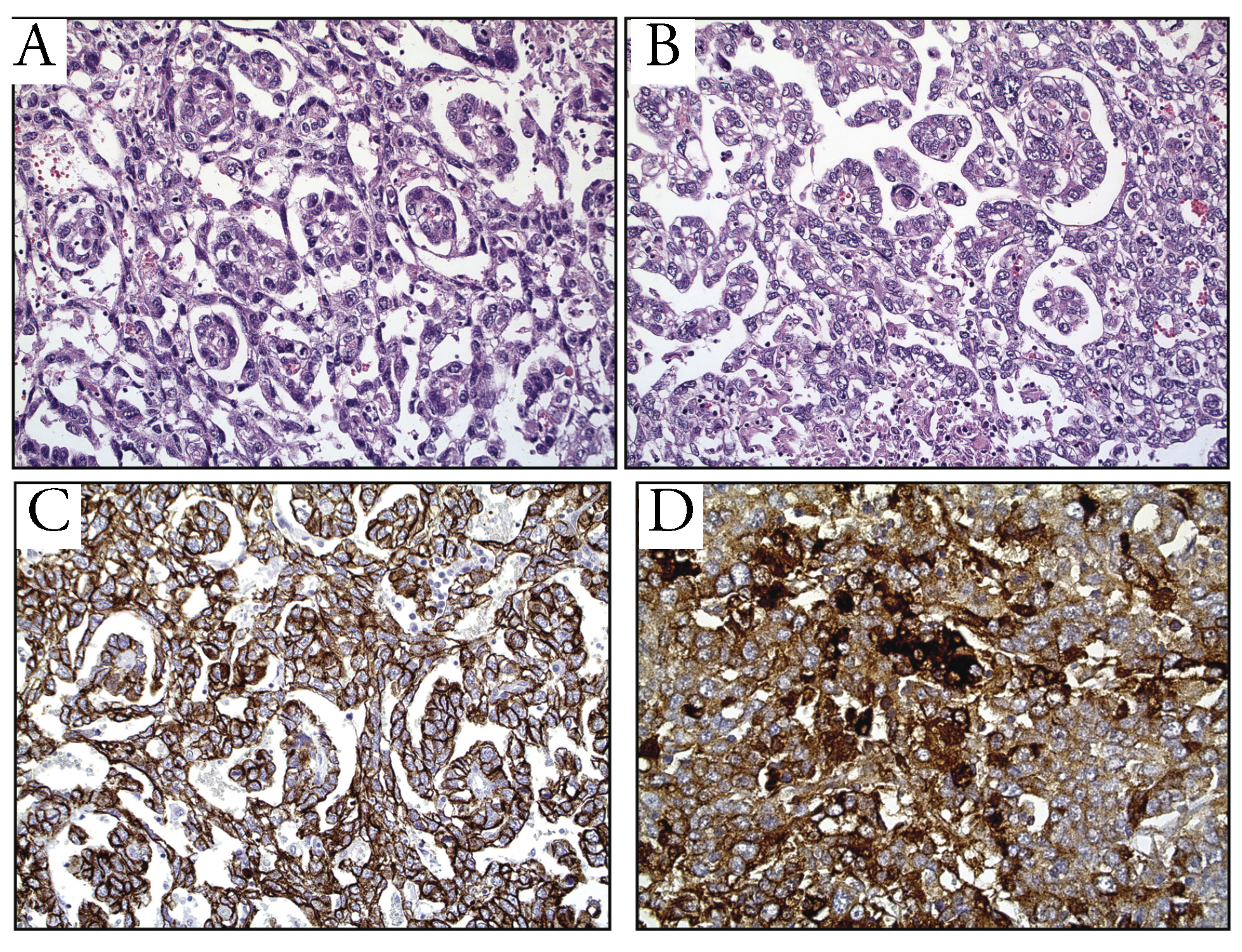
Discussion
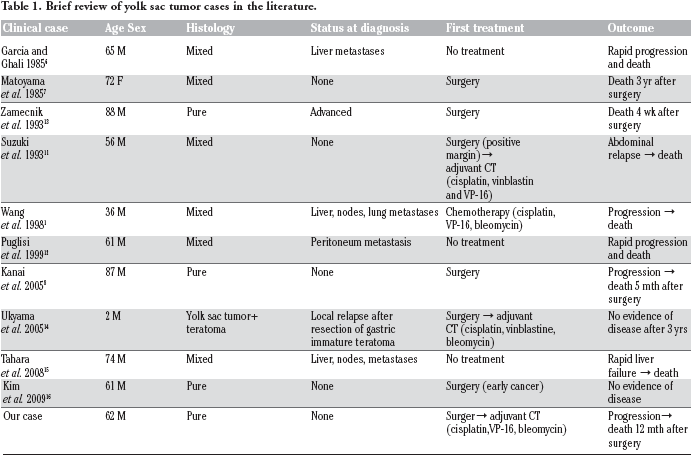
Gastric YST may affect elderly patients, as confirmed by our case, but clinical symptoms are most often unspecific and related to organ diffusion. Preoperatively α-fetoprotein is also a reliable tumor marker giving a well-defined histological feature at diagnosis. The first choice of treatment of localized YST is surgical resection despite a poor prognosis related to rapid diffuse relapse, and no conventional adjuvant or metastatic treatments are available. YSTs are germ cell tumors mostly found in the gonads. Extragonadal sites are reported in 20% of cases, occurring along the midline in the mediastinum, in the retroperitoneum, sacral area, and skull base. However, primary pure YST of the stomach is exceptional, with only very few cases reported in the literature 1–5 (Table 1). Gastric YST may also be accompanied by other neoplastic components including conventional adenocarcinomas, or other germ cell components such as choriocarcinomas and embryonal carcinomas.6,7 To the best of our knowledge, only six cases of pure YST of the stomach, with a median age of 65 years (range 36–87 yr), and five cases of YST combined with adenocarcinoma 8 have been reported. Generally high levels of α-fetoprotein are detected in the serum of patients with gastric YST. In our case this assay was performed only after complete surgical resection and its value was within the normal range.
Brief review of yolk sac tumor cases in the literature.
The origin of gastric YST is unclear, but involvement of migrating germ cells during embryonic development9,10 or multipotential neoplastic protoepithelial cells of the gastric mucosa 6 have been implicated. In combined variants of YST with conventional adenocarcinoma, α-fetoprotein was expressed strongly in the YST but not in the adenocarcinoma component, whereas the reverse held true for carcinoembryonic antigen. 11 A common derivation of combined tumors from a common ancestor has been suggested on the basis of the differential distribution of p53 nuclear accumulation in the YST and adenocarcinoma components. 12
The prognosis of gastric YST is generally poor and the standard therapeutic approach beyond surgery is still uncertain, with many patients experiencing widespread metastases at the time of diagnosis. Overall survival of published cases was one to seven months, with the exception of one 72-year-old patient without distant disease at diagnosis, who lived for a further three years.