
Abstract
We describe a rare case of a primary intracranial meningeal hemangiopericytoma (HPC) with late metastasis to the cervical spine. A 36-year-old woman had a left occipital lesion that was histopathologically identified as HPC. Fourteen years after resection, the tumor recurred and was treated with radiotherapy. Three years later, CT imaging showed a large mass in the liver consistent with metastatic HPC, and MRI of the cervical spine showed an extensive lesion of the C3 vertebral body. The patient underwent C3 corpectomy with en-bloc tumor removal and follow-up radiation with no local recurrence or other spinal metastasis for the following 4 years. Regardless of the subtype of spinal HPC, complete surgical removal and radiotherapy appear to be treatment of choice.
Keywords
Introduction
The term “hemangiopericytoma” (HPC) is used to describe a wide variety of lesions sharing certain morphological characteristics: a monotonous appearance at low-power examination, moderate to high cellularity, and numerous, variably thick-walled, branching ‘staghorn’ vessels. 1 HPCs demonstrating obvious malignant features generally behave aggressively; however, a small proportion of benign-looking lesions can recur and even metastasize. 1
Meningeal HPCs (M-HPCs) have different light microscopic, ultrastructural, and immunohistochemical features than meningiomas and are not considered variants of meningiomas. Their clinical behavior is more aggressive than that of benign meningiomas, and they have a strong tendency for local recurrence and extracranial metastasis.2–4
Spinal HPCs are significantly less common than intracranial M-HPCs. Despite the well-known but rare occurrence of HPC within the vertebral column, its natural history and management remain somewhat elusive. We describe a patient with primary intracranial M-HPC with cervical spinal metastasis that occurred six years after the primary lesion was detected. We also reviewed the literature to identify HPCs affecting the spine and to identify recognized treatment options.
Case Report
A 36-year-old woman visited the emergency room after experiencing several years of visual disturbances of increasing severity and frequency, nausea, dizziness, imbalance, hyperventilation, and numbness and upper extremity tingling. Imaging indicated that she had a left occipital lesion that enhanced on administration of a contrast agent. A complete resection was performed, and her symptoms improved. Pathological analysis of the resection was consistent with a meningioma.
The patient did well for fourteen years but redeveloped visual and neurological symptoms and was found to have local recurrence of the lesion. At this time, histopathological analysis showed the lesion to be HPC. Re-review of the pathological analysis done of the original lesion demonstrated that the tumor was a HPC that had been misdiagnosed as a meningioma. The patient underwent a course of radiotherapy to the left tentorium cerebellar region at a dose of 5400 cGy. Three years later, she developed right upper abdominal pain syndrome, and a computed tomography (CT) scan showed a large mass that filled the right lobe of the liver. She underwent a biopsy and a right hepatectomy, and the tissue was found to be consistent with metastatic HPC. Along with the metastasis in the liver, a lesion at the C3 vertebral body was found (Figure 1). On follow-up clinical evaluation, the patient had mild neck pain, with no motor deficits or sensory deficits.
A. Preoperative axial CT scan of C3. Note the destructive process involving the vertebral body. B. Preoperative coronal CT scan of C3.
Magnetic resonance imaging (MRI) of the cervical spine showed an extensive lesion of the C3 vertebral body that occupied approximately 90% of that vertebral body. It was directly adjacent to both vertebral arteries, and there was no evidence of epidural extension (Figure 2). An attempt was made to embolize the tumor, which had high vascularity, but the procedure was unsuccessful because there was significant arterial supply to the anterior spinal artery. None of the branches were large enough to be accessed safely for embolization. Two months later, the patient underwent a C3 corpectomy with removal of the tumor en bloc. To reconstruct the vertebral body, a titanium mesh cage, polymethylmethacrylate (PMMA), and an anterior cervical plate were used (Figure 3). 7 Follow-up radiation treatment of the cervical spine was administered with a total dose of 3750 cGy in 15 fractionated doses over 21 days. Clinical and imaging monitoring during the past four years has demonstrated no local recurrence or other spinal metastasis (Figure 4).
Preoperative T2-weighted axial MR image of C3. The hyperintense lesion is noted anterior to the spinal canal within the vertebral body of C3 adjacent to the left vertebral artery.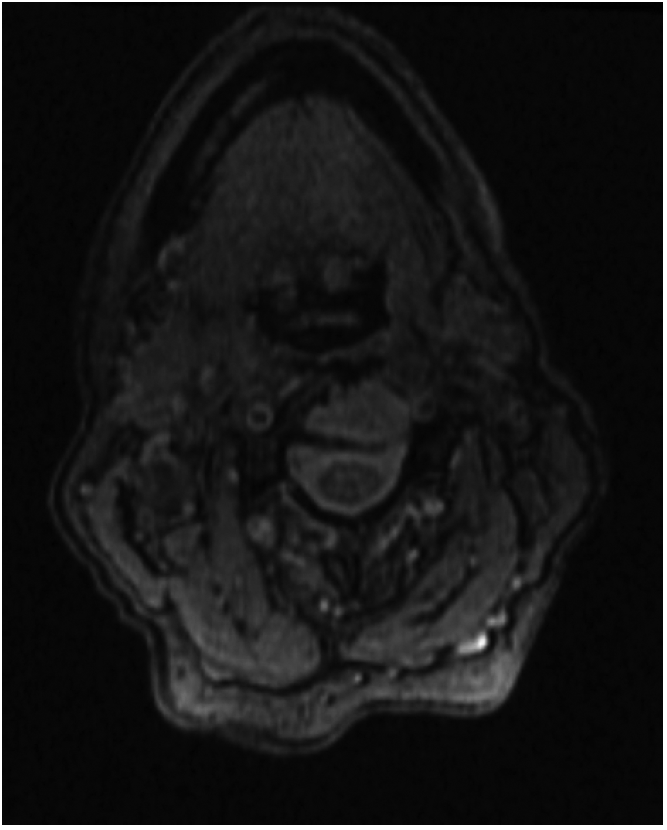
Postoperative sagittal CT of the cervical spine. A corpectomy of the vertebral body has been performed with the placement of a titanium mesh cage, PMMA, and an anterior cervical plate.
Postoperative T2-weighted sagittal MR image of the cervical spine. A corpectomy of the vertebral body has been performed, and the C3 vertebral body is distorted by the placement of a titanium mesh cage, PMMA, and an anterior cervical plate.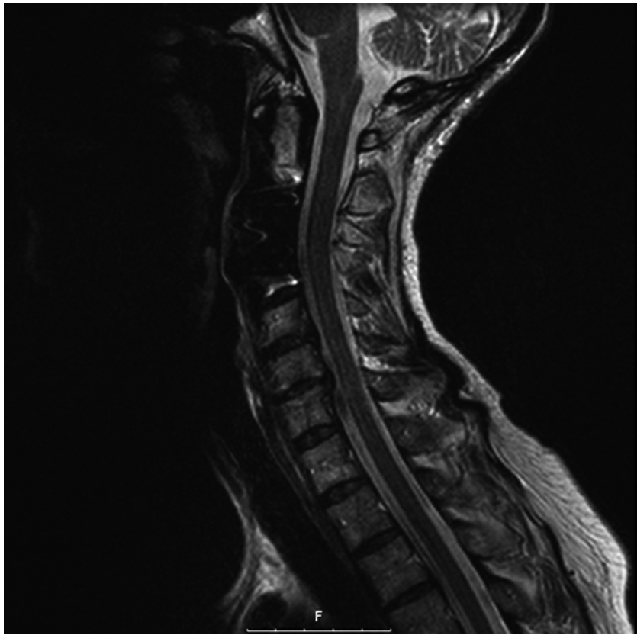
Discussion
HPCs are soft tissue tumors composed of capillary blood vessels with one or more layers of rounded cells showing features of pericytic differentiation. The thick-walled, branching ‘staghorn’ vessels are easily identified. Pericytic differentiation, which is more difficult to diagnose, has been based historically on the presence of elongated cell processes, pericellular basal lamina, plasmalemmal pinocytosis, and variable numbers of microfilaments. 8 Immunohistochemical analysis has shown that these tumors usually express muscle-specific actin, smooth muscle actin, and tropomyosin but are mostly negative for desmin and h-caldesmon.9,10
The clinical behavior of HPCs, especially extrapleural HPCs, is unpredictable. Approximately 10% to 15% of these tumors demonstrate malignant behavior in the form of recurrent or metastatic disease.11,12 Systemic metastases from intracranial HPCs have been reported. The specific criteria that define malignancy for HPCs include large tumor size (>50 mm), disseminated disease at presentation, infiltrative margins, high cellularity, nuclear pleomorphism, areas of tumor necrosis, and an increased mitotic index (>4 mitoses per 10× high-powered field).11–14 Nevertheless, the correlation between morphology and outcome is poor: some histologically malignant-looking lesions may behave benignly, and some morphologically innocuous lesions behave aggressively.1,11,13,15
Cases of spinal HPC are much less common than cases involving other anatomical locations. Intraspinal extradural M-HPCs and primary osseous HPCs are difficult to differentiate but are more frequent than intradural HPCs and secondary osseous HPCs. Thirty-one cases of extradural and primary osseous spinal HPC have been reported within the English literature (Table 1). HPCs of intracranial or extracranial primary sites that metastasize to the spine (Table 2) are much rarer.5,6,16 Intradural spinal HPCs (Table 3) are as rare as these latter two spinal HPC subtypes.
Reported cases of spinal HPC.
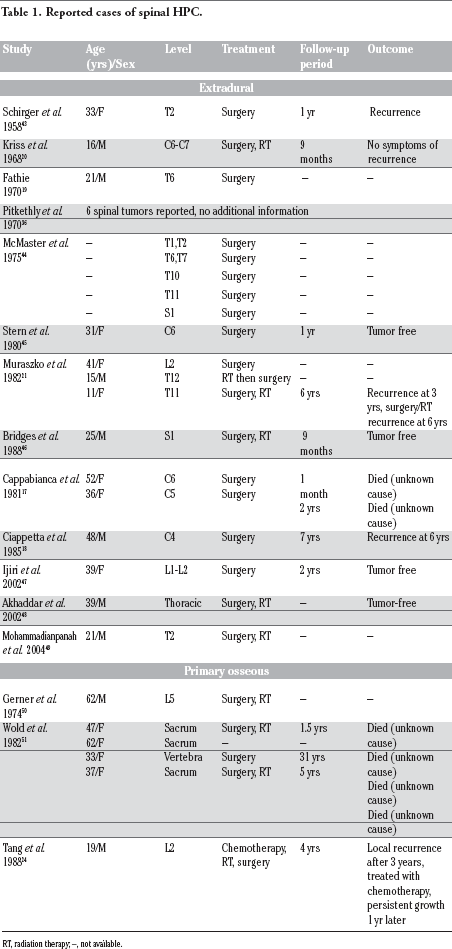
RT, radiation therapy; –, not available.
Reported cases of metastatic HPC to the spine.

RT, radiation therapy; –, not available.
Reported cases of spinal HPC.

RT, radiation therapy; –, not available.
We have separated extradural (intraspinal) from primary osseous HPCs according to their original case reports, although delineating them is often difficult. In reviewing the literature, we found that different clinical features have been observed in extradural M-HPC and primary osseous HPC. Extradural HPCs generally involve the middle and lower portions of the cervical spine. Often, but not always, these tumors demonstrate a dural attachment.17–21 Because of the involvement of the epidural space, radiculomyelopathy is a common finding.22,23 In contrast, primary osseous HPCs of the spine mostly affect the lumbosacral spine and have paravertebral extension 24 but do not result in neurological deficit. The most common complaints are pain and mass effect. 24
Spinal metastasis should be considered a possibility when a patient who has been treated previously for HPC presents with back or neck pain or pain accompanied by weakness. 25 Once symptomatic spinal metastasis is diagnosed, there is no satisfactory treatment modality to stop the fast and fatal progression. 25 Bone scintigraphy may be a useful screening tool to detect osseous metastasis early; however, a single negative scan may not be sufficient to confirm that there has been no bony metastasis. 26 In addition, gadolinium-enhanced MRI provides a very sensitive method of detecting spinal metastasis. For those patients who survive more than several years after the diagnosis of their primary HPC, aggressive spinal surveillance should be advocated. 25
Several long-term studies have documented the propensity of M-HPCs to recur locally or regionally within the cranial or spinal meninges.2,27–36 Results from the literature suggest that complete excision is more successful in preventing or delaying recurrence than is incomplete excision.2,27,31,34,37,38 Complete excision at the first operation significantly extended the average time before first recurrence from 43 months to 111 months. The five-year recurrence-free rate for those patients treated with complete excision was 72.7%, whereas that for those patients treated with incomplete excision was just 20.8%.
The surgeon should be prepared for a substantial amount of bleeding during tumor excision because of the high vascularity of HPCs. 16 This bleeding can lead to high surgery-related morbidity and mortality and can be the greatest hindrance to gross total resection. Preoperative embolization can be used to reduce blood loss. Thus, en bloc resection with extratumoral devascularization is the option most likely to reduce operative blood loss and possibly decrease the risk of recurrence; however, this may not be possible for those tumors with extensive premedullary portions. 16 When considering resection options, the surgeon should also be mindful that a piecemeal removal is associated with an earlier recurrence rate. 5
Even after en bloc resection, the possibility of recurrence necessitates close monitoring of the patient and consideration of adjuvant therapy. The length of survival for each patient also depends on the site and size of the primary tumor. 39 Tumors larger than 6 cm are associated with much poorer prognosis than are smaller tumors. 14 Outcomes for patients with intradural and extradural HPCs have been found to be similar. Even with the similar recurrence rates, however, disease-free survival was longer for those patients with an intradural lesion (average of 6 years before recurrence). 5
Although surgery alone offers local control of several years on average, the addition of postoperative radiotherapy (RT) to surgical treatment appears to be the best long-term treatment option for HPCs. 32 Using intensity-modulated RT and fractionated stereotactic RT with high radiation doses, the morbidity associated with adjacent organ damage, especially spinal cord toxicity, is minimized.40,41 Combs et al. 40 analyzed the use of high-precision RT in patients with HPC, including 2 spine cases. They demonstrated an overall survival rate of 100% at 5 years and 64% at 10 years for patients treated with a combination of surgical and RT approaches.
Radiosurgery and intensity-modulated RT can be considered in the setting of prior radiation, although the role of radiosurgery for metastatic spine disease is evolving because new technologies that deliver higher, more conformal doses of radiation could result in better local control. 42 The use of chemotherapy remains controversial, as most attempts have been disappointing.
Conclusions
Intradural, intraspinal extradural meningeal/primary osseous, and secondary metastatic osseous HPCs in the spine are rare and have only been infrequently reported. Regardless of the subtype, complete surgical removal and RT appear to be treatment of choice for HPC in the spine. Overall and progression-free survival times of patients with HPCs have continuously improved; however, the treatment of HPC is still unsatisfactory and remains a great challenge.
Footnotes
Acknowledgments:
we thank Kristin Kraus, M.Sc., for editorial assistance in preparing this paper for publication.