
Abstract
Hemangiopericytoma is a rare vascular tumor arising from pericytes and occurs very rarely in sinonasal region. A 48-year-old man with sinonasal mass presented with nasal obstruction and occasional epistaxis. Nasal endoscopy showed a readily bleeding mass in the left nasal cavity. Endoscopic removal of the mass was done. The histopathology came out to be hemangiopericytoma. The patient was kept on follow-up, and no metastasis or recurrence was seen in last 1 year. Hemangiopericytoma is a very rare vascular tumor. Surgery is the mainstay treatment of choice. A long-term follow-up is needed after surgery to rule out recurrence and metastasis.
Introduction
Hemangiopericytoma is a rare upper aerodigestive tract vascular tumor deriving from extracapillary cells called Zimmermann’s pericytes—modified smooth-muscle cells with mesenchymal origin in the periphery of blood vessels. 1
It may appear in any capillarized tissue, most frequently in retroperitoneum, pelvis and skeletal muscles of lower extremities. 2 Only about 15% are located in the head and neck region and in which <5% are found in nasal cavity and paranasal sinus. Hemangiopericytoma of the nasal region is usually more benign in nature with low tendency of metastasis but with a recurrence rate of approximately 25%. 3
This is the first reported case from Nepal. It is an uncommon sinonasal tumor. Reporting a rare case increases the knowledge of this rare disease, helps in understanding the beneficial and adverse effects of different interventions and overall aids in medical education.
Case report
A 48-year-old male came with a chief complaint of left-sided nasal obstruction and frequent episodes of bleeding from the same side for 6 months. No other nasal symptoms were present. Patient had unremarkable past medical and surgical history. Nasal endoscopy showed pinkish, smooth polypoidal mass between the left nasal septum and inferior turbinate. His blood parameters were normal. His pre-operative hemoglobin was 11 g/dL. The non-contrast computed tomography (CT) showed homogeneously hypoattenuating soft tissue density lesion occupying right mid-posterior nasal cavity and extending into the nasopharynx. There was widening of right posterior nasal cavity possibly due to bone remodeling. Contrast-enhanced computed tomography (CECT) scan showed mildly enhanced lesion, displacing medial wall of the right maxillary sinus and nasal septum (Figure 1).

Non-contrast computed tomography and contrast-enhanced computed tomography scan of nose and PNS. Mild enhancement seen on contrast-enhanced computed tomography.
The mass resection by an endonasal approach was planned under general anesthesia. Pre-operative embolization was not done because of lack of facility in our institution. Intraoperatively, voluminous smooth mass had been discovered extending to left nasopharynx, left nasal cavity and left maxillary sinus. The mass was removed completely (Figure 2).
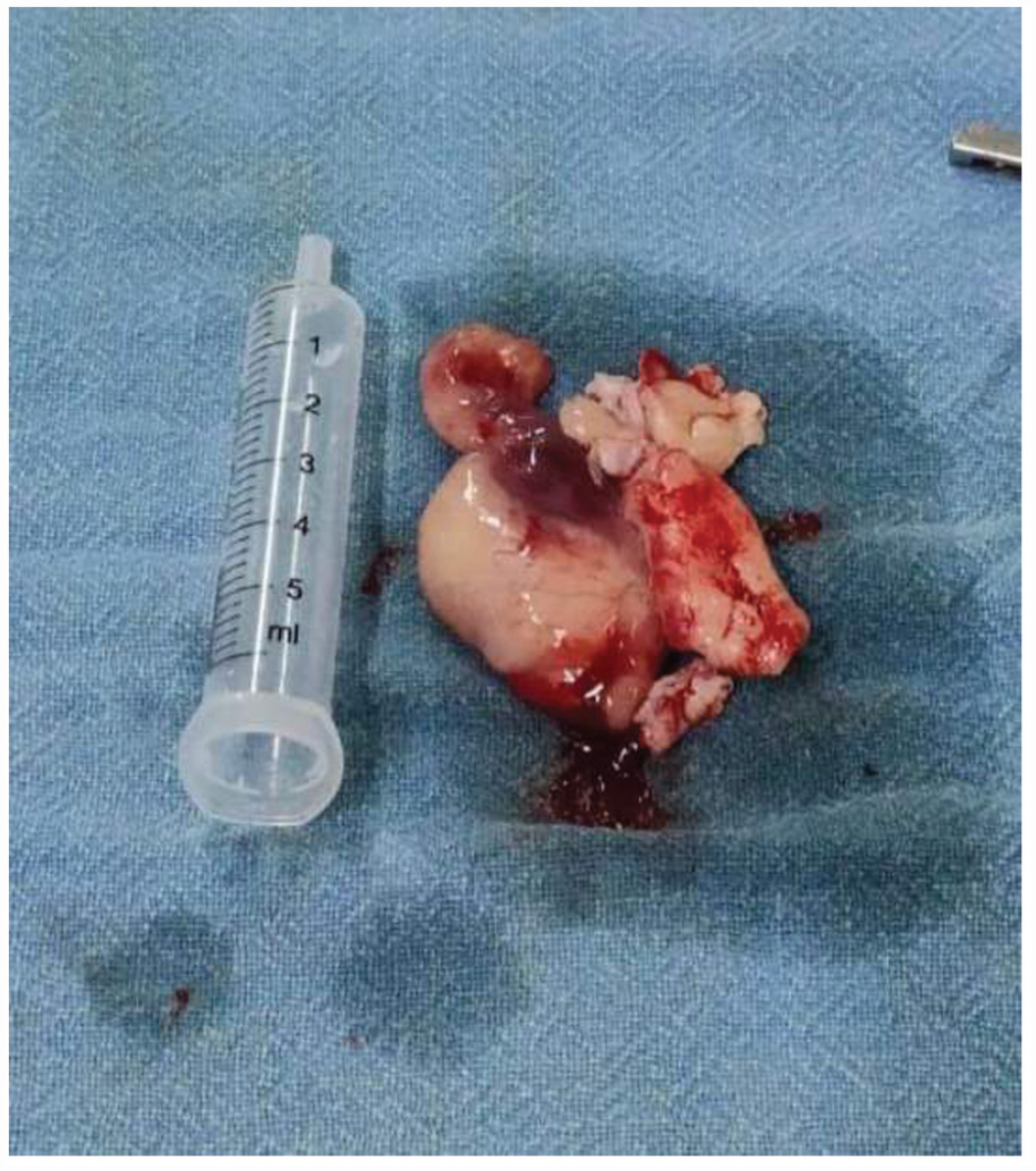
Gross specimen after endoscopic surgical excision.
On the histopathological report, the diagnosis of benign spindle cell neoplasm suggestive of solitary fibrous tumor was reported. The tumor cells showed lining respiratory epithelium with underlying stroma showing fascicles and sheets of spindle cells with intervening ropy collagen. The cells were round to ovoid in shape having moderate amount of cytoplasm with enlarged nuclei with granular chromatin. Focal areas showed branching thin-walled blood vessels lined by single layer of endothelium. Areas of necrosis or atypia were not seen. Mitotic figures were not seen. Immunohistochemical examination was done to confirm the diagnosis. The result showed CD34, S100, smooth muscle actin (SMA), K167 and CD99 staining was positive and CD31 and STAT6 staining was negative. The final diagnosis of sinonasal hemangiopericytoma was made (Figure 3).

Pathological section: respiratory epithelium with diffuse spindle cell proliferation and staghorn blood vessels in stroma.
The hospital stay of patient was uneventful. Neither intraoperative nor post-operative blood transfusion was needed. His post-operative hemoglobin level was 10 g/dL. The patient was discharged on the third post-operative day. Patient came for follow-up till 1 year. No any evidence of recurrence or metastasis was evident during the follow-up period.
Discussion
In 1942, the tumor was first described by Stout and Murray. 4 Hemangiopericytoma is a soft tissue tumor derived from mesenchymal cells with Zimmermann’s pericytic differentiation. It can be both benign and malignant in nature. Hemangiopericytoma constitutes only 3%–5% of all soft tissue sarcomas and about 1% of all vascular tumors. The head and neck incidence is about 15%. 4
There has been dispute regarding the use of term for the tumor, some authors prefer “intranasal hemangiopericytoma—like tumors” and others prefer “sinonasal hemangiopericytoma” due to strong bound with soft tissue hemangiopericytoma. 3 However, in 2005, the World Health Organization (WHO) classification of head and neck tumors proposed the term glomangiopericytoma due to their similarity with glomus tumors. Nowadays, in clinical practice, the term “hemangiopericytoma” for all tumors with hemangiopericytoma-like histology has become accepted. 5
Hemangiopericytoma can occur in any age groups, mostly in sixth to seventh decade of life. There is no gender predilection. 6 The etiology of the tumor is still unknown. Based on the patient’s medical history and clinical findings, factors such as trauma, long-term steroid use, arterial hypertension and hormonal or metabolic imbalance could be the predisposing risk factors. 7 However, these factors are regarded as obsolete in the contemporary literature.
Usually tumor is located in the nasal cavity and presents with epistaxis and nasal obstruction. 8 Pain is usually absent and if present should be regarded as a sign of local infiltration. 9 Other infrequent symptoms are vision impairment, headache and local swelling. Majority of the tumors grow rapidly so the history is of short duration. 10
During ear, nose and throat (ENT) examination, it can be often mistaken as inflammatory polyps. On examination the mass is pinkish to whitish in color and firm in nature. On contrast enchanced CT scan of paranasal sinuses, well circumscribed soft tissue mass can be seen without any bone erosion giving the differential diagnosis of nasal polyps, inverted papilloma, solitary fibrous tumor and lobular capillary hemangioma. However, in large lesions, bone erosion of nasal cavity, paranasal sinuses and adjacent orbital walls and skull base have been reported. 11
The diagnosis of hemangiopericytoma is based on the clinocoradiological and pathological findings. Based on cellular pleomorphism, mitosis and cellularity, these tumors are classified as low intermediate or high grade. Characteristics “staghorn” pattern is seen in sinonasal hemangiopericytoma but is not specific. Tumors consists of tightly packed cellular areas surrounding thin-walled branching blood vessels. Cells are ovoid to spindle shaped showing ill-defined cell boundaries. Immunohistochemical studies play an important role in strengthening the diagnosis. Vimentin and CD34 are considered the most reliable markers. 4 Immunohistochemistry (IHC) markers (CD34, S100, SMA, Ki67 and CD99) were immunoreactive in our patient.
The treatment of choice is wide-field excision with negative margins. 3 Endoscopic surgical removal was chosen for our patient, as it provided better overview and established more precisely the tumor insertion and its extension. Furthermore, it decreased the loss of blood, maintained the natural physiology of the nose and reduced the risk of damaging the lacrimal structures, and there was no post-operative scar. 3
Other treatment modalities such as chemotherapy, radiotherapy and immunotherapy are reserved for metastatic disease, unresectable and recurrent tumors. However, the efficacy of radiation therapy is doubtful as these tumors are considered to be radioresistant.12,13
The prognosis of these tumors is not definitively predictable. According to the literature, the tumor has been reported to have recurrence rate from 9.5% to 50%, with an average time of recurrence rate of 6–7 years. 14 However, recurrence has been even reported 26 years after tumor resection, so it is mandatory to have regular, lifelong surveillance of such patients. The primary factor in recurrent disease is an incomplete primary excision. 15
Conclusion
Sinonasal hemangiopericytoma is a rare vascular tumor. The recommended treatment is surgical excision of the tumor with a free resection margin. Nowadays, with few exceptions, resections can be conducted endoscopically. However, long-term follow-up is needed after surgery because of chances of recurrence and metastasis.
Footnotes
Author contributions
A.P. drafted the manuscript and performed surgery; S.R. performed surgery and also contributed in the manuscript by collecting photos of the specimen and CT scan. A.B. performed the pathological evaluation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Consent for publication
Written consent for publication was obtained from patient.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.