
Abstract
Background
Stunting is a global and national problem that can be detected at the age of 2. Therefore, before this age, promotion efforts must be conducted to prevent stunting risk factors in the future. This study aims to determine the effect of health education and infant's Therapeutic Group Therapy on stunting's risk factor: maternal postpartum depression in Indonesia.
Design and methods
This study employed a quasi-experimental design with a pre-test and post-test with a control group. This study employed a purposive sampling technique, with 96 respondents divided into two groups. Intervention group 1 consisted of 48 people who received health education, and group 2 consisted of 48 people who received health education and infant's Therapeutic Group Therapy. The data were collected using the Depression Inventory-II questionnaire with a bivariate analysis of the Wilcoxon test and frequency distribution.
Results
The results show that health education and infant's Therapeutic Group Therapy significantly influence the risky factors in stunting: maternal depression. It can be concluded that there were significant changes in maternal postpartum depression in intervention group 1 and intervention group 2, but in intervention group 2 who got Health Promotion and Therapeutic Group Therapy for Infants there was a bigger and more significant decrease.
Conclusions
Nursing action, infants’ Therapeutic Group Therapy, and health education are recommended to prevent risk factors for stunting: mother depression. The results of this study are expected to underlie the development of mental health promotion to prevent stunted against maternal depression and preventive programs. In addition, the research is expected to underly provision of curative and rehabilitative programs for stunted.
Introduction
Stunting is one of the most significant health problems, and it should not be ignored in society. 1 Stunting is a condition of failure to thrive naturally in children under five-years-old. It is due to the impact of chronic malnutrition and psychosocial stimulation and exposure to infections, especially in the first 1000 days of a child's life. 2 Toddlers experience the problem of stunting in the world and Indonesia. The World Health Organization (WHO) sets a limit of tolerance for stunting (short stature children) to a maximum of 20% or one-fifth of the total number of children under five. 3
Significance for public health
The prevalence of stunting in Indonesia is large. Stunting is a global and national problem that can be detected at the age of 2. Promotion efforts must be conducted to prevent stunting risk factors in the future. In Indonesia, there has never been an assessment related to maternal mental health conditions, including a history of depression in mothers and stunting stunting risk factor in baby with age 0-6 month. Depression experienced by mothers during pregnancy is one of the risk factors for causing stunting in children in the future. This study determined the effect of health education and infant's Therapeutic Group Therapy on stunting's risk factor: maternal postpartum depression in Indonesia. The results show that health education and infant's Therapeutic Group Therapy significantly influence the risky factors in stunting: maternal depression. Nursing action, infants’ Therapeutic Group Therapy, and health education are recommended to prevent risk factors for stunting: mother depression.
The incidence of stunting in children under five in Indonesia based on the 2013 Basic Health Research was 37.2% of the population. 4 While in 2018, Basic Health Research showed a decrease to 30.8% of the population or around 7 million children under five suffer from stunting, for babies under 2 years of age there are 28, 9% or 372,929 people. 2 Although there was a decrease in stunting incidence from 2013 to 2018, it shows that the number of stunting in Indonesia still exceeds the WHO. Stunting can be detected at 2 years old. Therefore, before the age, promotion, and prevention of risk factors must be conducted to prevent further stunting. The efforts can be started at pregnancy and before 2 years old. Prevention, as soon as when the baby is born in normal conditions, will reduce the incidence factor later.
Risk factors that affect stunting at 0-6 months of age are low nutritional intake, breastfeeding, nutrition for breastfeeding mothers, and the parenting. 4 Nutritional intake in infants is fulfilled through Early Initiation of Breastfeeding (IMD) and breastfeeding the baby with exclusive breastfeeding for the first 6 months and nutrition of nursing mothers. 5 Babies who get breast milk immediately after birth will have higher immunity; thus, they are more resistant to disease threats. 6 It is in line with a study by Laksono and Kusrini stated that in infants aged 0-6 months, food intake was fulfilled from the mother's exclusive breastfeeding. If it is not fulfilled, it can be one of the main factors causing stunting later. 7
The nutritional status of the mother also affects the breastfeeding of the baby. A study by Kominiarek shows that nutrition in postpartum mothers affects milk production. If breastfeeding mothers are malnourished, it will affect breast milk coverage because the body requires adequate nutrients. 8 Fulfillment of nutrition can be related to problems during childbirth, breastfeeding, or afterward, such as insufficient breastfeeding for nutritional intake; if there is no adaptive response, it can cause issues such as maternal depression. 9 Mothers who experience depression usually refuse to breastfeed their babies, are less responsive to baby cues and tend not to listen to health workers or their families’ advice.10,11 When a mother is depressed, she pays less attention to her health and her children's healthy development. Consequently, the children who do not get the fulfillment of nutrition will affect risk factors for incidence.
Research by Bennett et al. reports that parents’, especially mothers’, knowledge and mental health will affect the baby's growth and development. 12 Mothers who experience mental problems, especially depression, will cause children's growth, development, cognitive issues, and psychosocial issues. 6 Therefore, it can be interpreted that mothers who experience depression can cause children's lack of stimulation.
Promotional and preventive efforts to improve the family's ability to support the health needs, growth, and development of family members, especially parents who have babies, because family is an important part that can affect individuals’ health status.2,13 These efforts include Therapeutic Group Therapy (TKT), a type of group therapy that allows members to share experiences, help one another, find ways to solve problems and improve their abilities. 1 Research by Restiana et al. proves that TKT in infants can improve maternal cognitive and psychomotor abilities and infant trust. 14 Meanwhile, research by Soeli, Keliat, and Ungsianik shows that Therapeutic Group Therapy improves infant abilities and infant confidence. 15 However, research on the effect of infant TKT and health education on stunting, nutrition, parenting, and depression on risk factors for stunting in infants has never been conducted. This research will be conducted in Indonesia because the malnutrition problem of stunting is an Indonesian infant's frequent problems and still has a very high incidence and needs attention.
Design and Methods
This study employed a quasi-experimental design, a pre-test, and a post-test with a control group. The quasi-experimental design aims to observe the results of the intervention by measuring the conditions before the intervention was given, then after the intervention was carried out measurements were made to obtain comparative data. Inclusion criteria in this study: Parent (mother as the baby's primary caregiver, willing to be a respondent in research, respondents are able to read and write, respondents are able to communicate well) and baby with age 0-6 month.
The sampling employed a purposive sampling technique, with 96 respondents who were divided into 2 groups. Intervention group 1 (control group) consisted of 48 people who received health education about stunting, nutrition, parenting, and maternal depression. In the second intervention group (intervention group), 48 people received Therapeutic Group Therapy for infants and health education about stunting, nutrition, parenting, and maternal depression. The Therapeutic Group Therapy for babies consisted of 6 sessions: stimulation of the motor development, cognitive and language aspects, emotional and personality, and moral, spiritual, social, and monitoring evaluation of experiences and benefits. Each session was conducted for 45-60 minutes. This study has met the ethical considerations and was approved by the Ethics Committee of the Faculty of Nursing, Universitas Indonesia (Permit ID: NKB-3451/UN2.RST/HKP.05.00/2020).
The data were collected by using the Edinburgh Postpartum Depression Scale (EPDS) questionnaire. This questionnaire was adopted from Ratu Kusuma's dissertation at 2017 with the title “The Effectiveness of the Ratu's Postpartum Depression Prevention Model on Prevention of Postpartum Depression” which has been tested for validity and reliability. 11 This questionnaire is not only used to measure postpartum depression but also pregnancy depression with 10 statements in which each statement has 4 answer choices with a score range of 0-3 then the scores from each statement are added up and categorized <10 = not depressed, and 10 = depression. The fulfilment of the questions follows the instruction that the respondents must reminisce the condition of their pregnancies. This research was conducted online with a Google form distributed to the public, and the link was sent via the WhatsApp application. Mothers who have babies and met the research criteria were involved as respondents and filled in the questionnaire. The researchers monitored respondents in each group through the WhatsApp group, provided workbooks, and distributed educational flyers about infant development tasks and stimulation.
The procedure for conducting research in groups 1 and 2 can be seen in detail in Figure 1
Data were analyzed using statistical software Univariate analysis in the form of proportional distribution was carried out on all variables. This result was analyses with Wilcoxon test of bivariate analysis, and frequency distribution.
Results
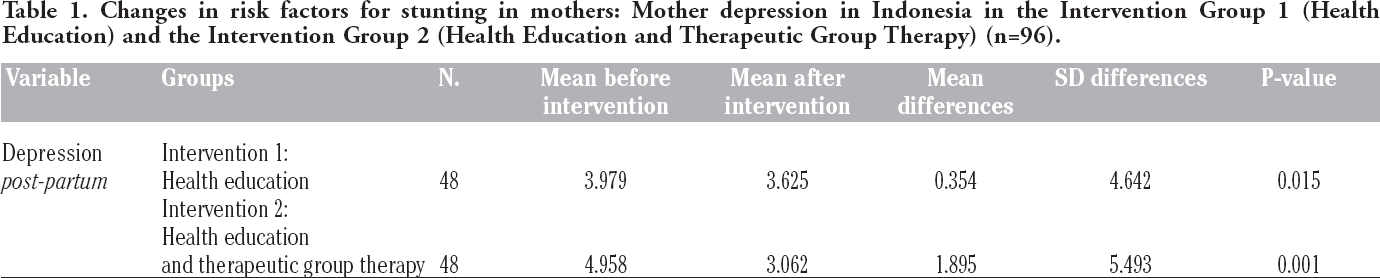
Maternal stunting risk factor changes, including maternal depression in the intervention group 1 before and after receiving health education about nursing action and intervention group 2 before and after receiving health education and TKT for babies were analyzed using the Wilcoxon test. The data of maternal postpartum depression were not normally distributed (Table 1).
Table 1 shows that mothers’ postpartum depression in the intervention group 1 after receiving nursing action for health education has decreased from 3.979 (8.84%) to 3.625 (8.05%) with a difference of 0.354. Meanwhile, the analysis results reveal a significant decrease in mothers’ postpartum depression score in the intervention group 1 after receiving health education nursing action (p<0.05). On average, the mothers did not experience postpartum depression. The statistical test results in intervention group 2 show a decrease in the average value of postpartum depression for mothers from 4.958 (11.02%) to 3.062 (6.8%) with a difference of 1.895. The analysis results discover a significant decrease in mothers’ postpartum depression score in intervention group 2 after receiving health education, and therapeutic group therapy for infants (p<0.05); the average mother did not experience postpartum depression. It can be concluded that there were significant changes in maternal postpartum depression in intervention group 1 and intervention group 2, but in intervention group 2 who got Health Promotion and TKT for Infants there was a bigger and more significant decrease.
Changes in risk factors for stunting in mothers: Mother depression in Indonesia in the Intervention Group 1 (Health Education) and the Intervention Group 2 (Health Education and Therapeutic Group Therapy) (n=96).
Based on the data analysis for postpartum depression categorical mothers in Indonesia, Table 2 shows that after receiving health education in intervention group 1, mothers who did not experience postpartum depression increased from 40 (83.33%) to 44 (91.67%). In comparison, mothers who did not experience postpartum depression, but experienced mild depression decreased from 6 people (12.5%) to 4 people (8.33%). Mothers who experienced moderate depression experienced a decrease from 2 people (4.17%) to none. Mothers who experienced depression decreased from 2 people (4.17%) to none. Whereas mothers in group 2, who received health education, and therapeutic group therapy for infants, did not experience postpartum depression and increased from 39 (81.25%) to 45 (93.75%). Mothers who experienced mild depression decreased from 4 people (8.33%) to 3 people (6.25%). None of the mothers experienced moderate depression or major depression.

The implementation procedures.
Changes in the frequency and percentage of Indonesian mother's depression after receiving health promotion and therapeutic group therapy (TKT) for infants (n=96).

Discussion
The group's maternal depression after receiving health education (Group 1) significant decreased from 8.84% to 8.05%. Maternal postpartum depression after receiving health education nursing action regarding stunting, nutrition, parenting, and maternal depression, and therapeutic group therapy for infants (Group 2), significant decreased from 11.02% to 6.8%. Maternal postpartum depression after receiving health education nursing measures about stunting, nutrition, parenting, and maternal depression, and therapeutic group therapy for infants showed that most of the mothers did not experience postpartum depression with significant changes. The category of maternal postpartum depression in Indonesia after receiving health education nursing action and therapeutic group therapy for infants shows mothers who do not experience postpartum depression increase. Moreover, there are no mothers who experience moderate depression or major depression.
Efforts to reduce the level of maternal depression are conducting by providing health education and discussion. Depression prevention starts with recognizing the definition of depression, depression risk factors, impact, and prevention. Moreover, the provision of depression prevention education in research is complemented by nutrition education for mothers and babies, parenting styles, and health education related to stunting. These three types of education will complement each other because the incidence of depression can be related to stunting. Stunting can be prevented by increasing the intake of good nutrition for mother and baby and providing the best parenting styles formed in the family. This education also grows respondents’ understanding of stunting prevention through the mother and baby and their environment. The respondents’ depression significantly decreased after receiving educational nursing action, but they had not reached the maximum score. The respondents received depression prevention, and one of which is stress management. This effort is necessarily given because mothers with depression usually refuse to breastfeed their babies, are less responsive to baby signals, and tend not to listen to health workers’ or their families’ suggestions.11,16 When a mother is depressed, she ignores her health and her baby's health and development. Consequently, her child does not get nutrition and is at risk of stunting.
The mother's negative thoughts frequently arise due to internal and external factors. The internal factors include adapting the mother to physiological changes 17 and psychosocial changes. 18 Other factors include adopting an unhealthy lifestyle, poor healthseeking behavior, inadequate physical and emotional care, and inadequate-psychosocial stimulation for babies. 9 When a mother is depressed, she ignores her health and her baby's health and development. Consequently, the child does not receive adequate nutrition and is prone to an incident.
Providing efforts to prevent stunting was combined with conducting infant's therapeutic group therapy. The researchers monitored respondents in each group through the WhatsApp group, provided workbooks, and distributed educational flyers about infant development tasks and stimulation. As a result, the mothers could relearn more what the researcher delivered. TKT for babies is carried out to improve the family's ability to meet the health needs, growth, and development of family members, especially parents who have babies, because family is an important element that can affect individuals’ health status.2,13 Therapeutic group therapy is a therapy group that allows members to share experiences, help one another, find a solution, and improve their abilities. 1 TKT has improved infant development. This enhancement of developmental abilities supports the babies’ health and will prevent them from any disease, and one of which is child malnutrition. 19 Preventing maternal depression from an early age is necessary to improve babies’ development and future growth. This study states that low interaction between mother and baby increases maternal postpartum depression and stunted infants’ growth. 17 Therefore, promotion and prevention efforts are compulsorily conducted.
Conclusions
The results show that the health education about nursing action regarding stunting, nutrition, parenting, and maternal depression and the Therapeutic Group Therapy for infants have significantly influenced the risk factor for stunting: maternal depression. Therapeutic Group Therapy about nursing measures for infants and stunting health education about nutrition, parenting, and maternal depression are highly recommended to prevent stunting risk factors: maternal depression. The results of this study are expected to underlie the development of mental health promotion to prevent stunted against maternal depression and preventive programs. In addition, the research is expected to underly provision of curative and rehabilitative programs for stunted. It is necessary to collaborate with the health office and Puskesmas in Indonesia to include health education on stunting, nutrition, parenting, and maternal depression and infant TKT in the Posyandu program to be used as an early promotive and preventive effort against stunting, in infants it is hoped that with this collaborative action, mental health improvements for mothers and babies will continue to increase.
Footnotes
The authors declare no potential conflict of interest.
Acknowledgments
We would like to thank the Director of Research and Development who has granted the funding for the 2020 International Indexed Publication (Publikasi Terindeks Internasional) of Universitas Indonesia. We also thank to the entire respondents who participated in this research.