
Abstract
Mental health is a major public health concern in China. Help-seeking behavior typically does not involve professionals. Aim of the study was to assess Shanghai women’s care-seeking behavior for common mental health disorders. Using an online survey, fielding questions regarding perinatal mental health status and help-seeking behavior. A total of 487 women participated. One fifth of participants reporting badwell-being did not seek help for mental distress. A total of 82.2 percent seek online support. A majority entrusted in family and avoided professional contact. Mother-in-laws were the least trusted source of support. Shanghai women avoid seeking professional help for mental health issues. Friends, spouses, and online resources are preferred venues.
Background
By 2025, an estimated 39.6 million years of healthy life will be lost due to mental illnesses in China annually as calculated using the Disability-Adjusted Life Years (DALY) index (Charlson et al., 2016). Phillips and colleagues investigated the mental health status in four provinces in China and found an adjusted 1-month prevalence of 17.5 percent for any mental disorder, 6.1 percent for mood disorders, and 5.6 percent for anxiety disorders (Phillips et al., 2009). In 2010, there were 757 mental health facilities and approximately 20,480 psychiatrists in China, far below the required numbers (Liu et al., 2013). A large majority of psychiatric professionals in China work in specialized hospitals with a skewed geographic distribution. The number of mental health workers per 100,000 residents is lower in China than in other upper-middle-income countries, and the range of professionals who provide mental health services is narrower. This has created a significant unfilled need (Shao et al., 2015). Training of licensed physicians and registered nurses working in mental health facilities in China is often lacking. In all, 29 percent of physicians have only a technical school degree and 14 percent have no academic degree. A total of 46 percent of the nurses have no post-vocational qualification (Jacob et al., 2007; Shao et al., 2015). In addition, there is only a negligible number of clinical psychologists and psychiatric social workers in China. The thin rank of mental health professionals compared with that of other medical professionals is in part due to low pay, as well as transference of the stigma associated with mental illnesses to those who work with mental health disorders (Chen, 2012). The Chinese urban health care system is organized into three tiers. Community health centers provide preventive services, medical treatment, and health care. District hospitals serve as secondary general hospitals and points of referral, while tertiary general hospitals provide advanced care and teaching duties. To promote high-quality medical care, a large number of comprehensive large-scale hospitals have been established. These include specialized hospitals such as mental health hospitals and obstetric centers (Park et al., 2005; Zhang et al., 2013; Zhou et al., 2015). The three-tiered system is fully developed only in large urban centers such as Beijing and Shanghai. Most localities in China are lacking community mental health workers of any kind.
Among individuals with any diagnosis of mental disorders, 91.8 percent never seek help (Liu et al., 2011). For psychotic disorders, 27.6 percent never seek help and 12.0 percent see non-mental health professionals only (Phillips et al., 2009). The World Health Organization’s (WHO’s) Mental Health Gap Action Program (mhGAP) recommends psychological treatment as first-line interventions for common non-psychotic mental disorders, a treatment for which China lacks availability (Keynejad et al., 2017; Schwank et al., 2018; WHO, 2015a). Recently, mental health has received increasing attention in China with a main goal of the 2013 mental health law to expand access to mental health services, including services during the perinatal period. These goals are in line with the WHO Sustainability Goals 4 and 5, relating to the health of mothers and children, which cannot be attained without attention to maternal mental health (Fisher et al., 2011). High-quality data on mental health problems in the perinatal period is needed, especially at the local level, to make pregnancy safer for women in low- and lower-middle-income countries (Fisher et al., 2012).
A recent systematic review on Chinese people’s care-seeking behavior for common mental health disorders concluded that the general population, as well as people with mental health disorders, described structural and attitudinal barriers in seeking help (Hsu et al., 2019). Various studies explained the prevalence of common mental health disorders among Chinese citizens and the lack of help-seeking behavior, resulting in extraordinarily low rates of diagnosed patients. The prevalence ratio of undiagnosed/diagnosed generalized anxiety disorder (GAD) is only 0.5 percent of GAD patients reporting a diagnosis (Yu et al., 2018). The perception and awareness of mental health among Chinese is very limited as a semi-structured interview study described, none of the participants could explicitly define mental health (Lu et al., 2015). Similar low prevalence rates were also found for patients currently using prescription medication for depression, only 8.3 percent were diagnosed (Gupta et al., 2016).
Postpartum depression (PPD) in China has a pooled prevalence of 14.7 percent nationally and 11.8 percent in Shanghai (Qian and Yan, 2013; Wong and Fisher, 2009; Yu et al., 2018). The mental health status of 6024 pregnant women were investigated when they enrolled to the services of the ObGyn hospital of Fudan University from September 2015 to August 2016, wherein 24 percent and 9.5 percent had symptoms of depression and anxiety respectively (Qiao et al., 2009; Zhang et al., 2019). Prevalence of PPD is considerably higher in women from the one-child generation (Xiong et al., 2018). There is some evidence that women without siblings are more likely to be affected by negative mood states such as depression, anxiety, and fear (Tseng et al., 1988). This is possibly due to an increase in early maladjustments leading to depression and anxiety in adulthood, as a consequence of being part of the one-child generation (Xiong et al., 2018). Perinatal psychiatric disorders are the leading cause of maternal morbidity and associated with serious, long-term consequences for maternal mental health (Howard et al., 2014; Stein et al., 2018). Previous research has identified a need for structural changes in mental health care services, especially for perinatal mental health problems and common mental disorders (CMDs), wherein increased use of services, better treatments, and service expansion are seen as equally important (Chen, 2018; Phillips et al., 2009).
Epidemiological research shows that women in large urban agglomerations are at increased risk of developing CMD (Huang et al., 2019). Concerns about the burden of mental disorders and their association with urbanicity have been intensified; however, little is known about the extent of these issues in megacities such as Shanghai (Huang et al., 2019). In accordance with tradition, Chinese families commonly include parents-in-law living and sharing a household with the new parents after childbirth. This living arrangement has been postulated as a risk factor for PPD among Chinese women in the perinatal period. In this study, our survey sought to better understand urban Chinese women’s care-seeking behavior for mental health problems, their perception of health care, and to whom they disclose (Schwank et al., 2019b).
Method
Design and setting
An online survey study was conducted using the local social media platform WeChat. The study was based in Shanghai municipality, encompassing the largest metropolitan area in China (Shanghai Bureau of Statistics, 2014).
Selection of participants
Inclusion criteria: Urban Mainland Chinese adult women living in Shanghai, of reproductive age, with experience of pregnancy or childbirth, and fluent in speaking and reading standard Mandarin Chinese. Study participants were invited via WeChat using a snowball technique as previously described (TenHouten, 2017). The choice of women of reproductive age was selected, due to the recent implementation of the two-child policy, affecting women born during the one-child policy, who are now given the reproductive choice of having two children (Schwank et al., 2018).
Data collection
This study was performed during the first half of 2019 through an app-based survey. The questionnaire was developed by our research team and based on results from the research group’s prior qualitative investigations with key perinatal health professionals and Shanghai women in child bearing age. Further research on childbirth and maternal health that used self-report questionnaires on help-seeking behavior and women’s experience of the perinatal period was integrated (Chen, 2012; Schytt and Hildingsson, 2011). Self-reported mental health status was estimated through a retrospective 12 months assessment adapted from the WHO Composite International Diagnostic Interview (CIDI)–based questionnaire used by Shen and colleagues (Shen et al., 2006). We asked the women to rate their mental health status during the past 12 months on a scale from 1 to 10, from “very bad” to “very good.” This global measure of the women’s mental health status was used to dichotomize the sample into two groups, regarding their feeling of being mentally healthy or having bad well-being. The dichotomization into a “healthy” and “bad well-being” group followed previous research using women’s self-report on pregnancy and birth outcomes (Chen, 2011, 2012; Schytt and Hildingsson, 2011). The participants received information disclosures about the study via the survey, and gave consent with their participation. The online survey contained 13 closed and one open-ended question. The closed questions were selection based, except for Question 1, based on a 10-score Likert scale, listed in Supplementary Appendix 1.
Study participants were recruited via the ObGyn Hospital of Fudan University, the Shanghai Women’s and Children’s Health Center, and the Chinese American Psychoanalytic Alliance (CAPA). The survey was sent out to participating women by a survey function in WeChat, a ubiquitous Chinese social media platform with more than 1 billion monthly active users (Statista, 2019). The platform requires its users to verify accounts through personal verification with a government-issued ID number.
Ethical approval
Ethical approval was obtained from the Ethics Committee in Stockholm (IRB No. 2018/1041-31) and of the Obstetrics and Gynecology Hospital, Fudan University (IRB No. 2018-51-X1).
Analysis
Statistical analyses were performed using SPSS Statistics v25.0 (SPSS, Inc., Chicago, USA). Continuous variables were analyzed by means and standard deviations, and categorical variables were analyzed by number and frequency. Statistical significance was set at a p value of p < 0.05. Binary logistic regression analysis was used to identify the association between explanatory variables and overall mental health status dichotomized into healthy and bad well-being. The women’s overall mental health status was estimated by a range from score 1 to 10 and dichotomized into “healthy” and “bad well-being” with a cut off at 4. Meaning that women scoring between 1and 4 were considered as experiencing bad mental well-being and women scoring 5–10 were considered as mentally healthy. The groups are labeled as “healthy” and “bad well-being” in the results in accordance with the self-reported estimates.
Results
Out of 529 successfully completed survey answers, 487 met the inclusion criteria. Participants’ ages ranged from 19 to 57 years, with a mean age of 35.15 ± 5.42 years. A majority were between 25 and 35 years old (53.6%). Most participants had one child (77.6%) and almost all (95.7%) had one or more university degrees. Educational attainment differed significantly between healthy and bad well-being groups (p = 0.002), with the healthy group having higher percentage of higher education (96.6%) compared with the bad well-being group (88.5%). The healthy group further earned significantly more (p = 0.024), which can be expected, considering the higher education level of that group. There was a statistically significant association between age and mental health status (p = 0.013). The group with the highest amount of bad well-being participants was the group aged between 25 and 35 years (Table 1).
Socio-demographic variables among Shanghai women (n = 487).

SD: standard deviation.
Women’s overall mental health status
The majority of the participating women were healthy, with 89.3% reporting a score of 5 and above. The age group 25–35 years reported higher levels of bad well-being (13.1% vs 7.3%) compared with the 35 years and older group (p = 0.013). There were too few participants in the >25 years group to draw conclusions, although two out of five did report bad well-being (Table 2).
Overall mental health status distribution.

Overall mental health status classified as reporting bad well-being 1–4, healthy 5–10.
Factors associated with women’s overall mental health status
Fifty-two women reported an overall mental health status 4 or lower and were therefore classified as having bad mental well-being. We analyzed related factors affecting their overall mental health status using binary logistic regression. Three variables including pregnancy/giving birth, general help seeking for mental health problems, and help seeking from professionals entered the final regression model. Participants with lower mental well-being considered pregnancy/giving birth as having affected their mental health status more (p = 0.008; aOR: 2.59; 95% CI: 1.28–5.24). They were less likely to seek help for their mental health problems (p = 0.003; aOR: 0.29; 95% CI: 0.13–0.66) but did express a higher likelihood to seek help from professionals (p = 0.001; aOR: 2.98; 95% CI: 1.59–5.58) compared with healthy participants (Table 3).
Logistic regression analyses of factors affecting overall mental.
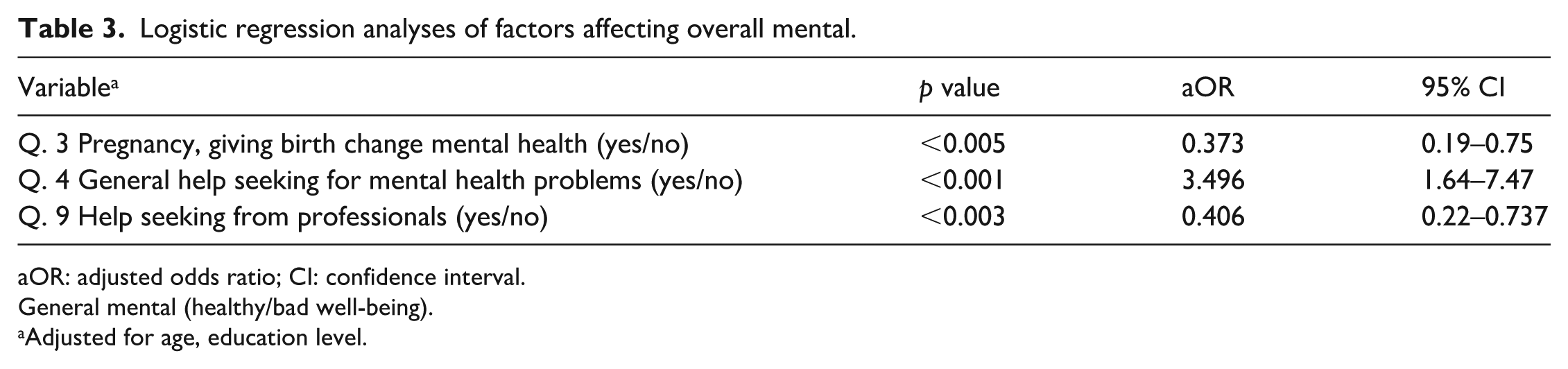
aOR: adjusted odds ratio; CI: confidence interval.
General mental (healthy/bad well-being).
Adjusted for age, education level.
Factors associated with women’s trust to share mental health problems
A high proportion of participants (37.2%) expressed trust in their friends when needing to share emotional problems and mental distress. There were no significant differences in the healthy group (38.4%) compared with the bad well-being group (26.9%). Spouses represented the second preference to turn to for help and emotional support (36.1%). Healthy women sought help from their spouses at a similar rate (37.5%) compared with the bad well-being group (25%). Lower number of care-seeking from friends and spouses in the bad well-being group were not statistically significant, although the survey showed a significant difference in the overall propensity to not seek help at all in the bad well-being group (21.2%) compared with the healthy group (7.1%; Table 4).
Logistic regression analyses of factors affecting trust to share mental health problems.
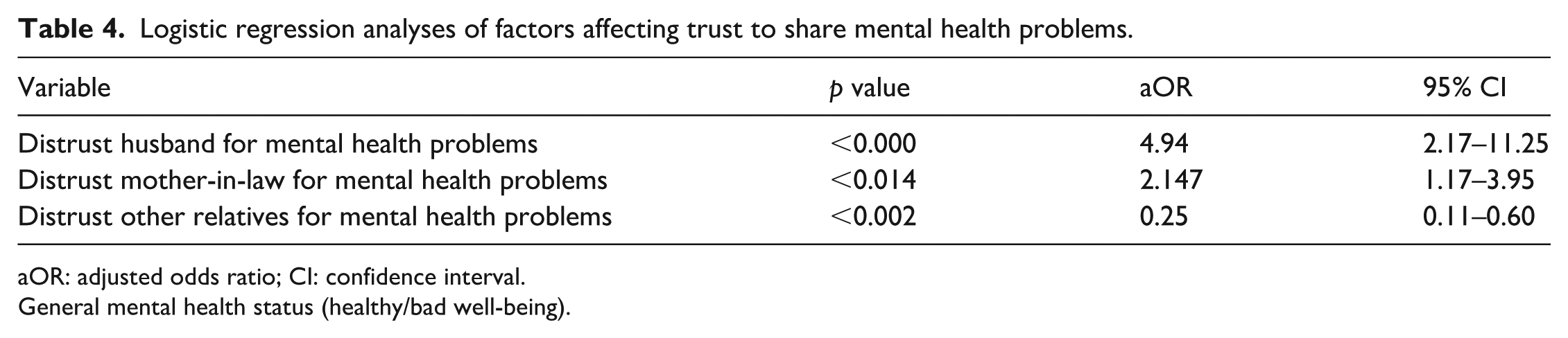
aOR: adjusted odds ratio; CI: confidence interval.
General mental health status (healthy/bad well-being).
Participants with self-reported bad mental well-being were significantly more likely to be distrusting of their spouses in matter pertaining to mental health problems (aOR: 0.21; 95% CI: 0.09–0.51). The same group further distrusted their mother-in-law to a significantly larger extent than did the healthy group (aOR: 0.41; 95% CI: 0.86–2.08). The reverse was seen with regard to other relatives, wherein healthy participants considered other relatives less trustworthy than reported by the bad mental well-being group (aOR: 4.39; 95% CI: 1.79–10.77; Table 5).
Logistic regression analyses of factors affecting distrust to share mental health problems in mental bad well-being women.

General mental health status (healthy/bad well-being). QQ: quick questions, a WeChat function.
Adjusted for age, education level.
Preference for type of professional mental health care
The majority of the women, responded to the hypothetical question, if they would seek professional help, what kind of professional help this would be. The women could choose from a range of options and most of the participants had a clear preference for reaching out to community health centers for their mental health problems (71.3%). The distribution was similar in both groups; (72%) of the healthy and (65.4%) of the bad well-being group, both preferred to visit a community health center for their mental health problems. General hospitals were the second preference for the entire study population (11.5%), the healthy group (11%) and the bad well-being group (15.4%). The preference to seek help at a mental health hospital (7.6%) or an obstetric hospital (5.7%) were also comparable between groups and less popular overall.
Attitude toward Internet mental health care services
The study population had a high preference for access to Internet resources (82.8%), with no difference between groups at 83% and 80.8%, respectively, for the healthy and bad well-being groups. There was a high preference rate for WeChat subscriptions (42.1%) as form of online support. The second choice was online consultations which (29.8%) of all women would access, if available. General WeChat groups were a much less popular choice at 9.9% (Table 6).
Distribution of preference for type of professional mental health care (%).

QQ: quick questions, a WeChat function.
Discussion
Prior research has shown that over 70 percent of Shanghai women do not seek help for perinatal mental health problems (Schwank et al., 2018). A similar pattern is seen in the general population, and low help seeking behavior is leading cause of lack of timely diagnosis and appropriate management of mental health disorders and may be associated with significant morbidity and mortality (Phillips et al., 2002; Shen et al., 2006). A majority (80%) of the survey participants stated a preference and lower threshold for seeking information and counseling provided via online resources such as WeChat, rather than seeking help from health care professionals (Schwank et al., 2018). Limited availability of affordable mental healthcare services, inadequate number of qualified and competent mental healthcare professionals, and social stigma associated with mental illness may have contributed to the stated preferences. Mu et al. (2019) and Xiong et al. (2018) found that the one-child generation suffers higher incidences of PPD and anxiety. The development of PPD in women from one-child families is therefore an important public health concern that is liable to expand as large age cohorts of only child individuals come of age and have children (Xiong et al., 2018).
Factors associated with women’s overall mental health status
A majority of our survey participants reported that pregnancy and/or giving birth had impacted their general mental health status. Both groups reported low likelihood to seek help for mental health problems. The low help seeking behavior in China is a continuing problem and attention to this phenomenon is of vital importance to improve mental health care on a wide scale (Charlson et al., 2016; Chisholm et al., 2007; Hot Topic: No Global Health without Mental Health, 2015).
Factors associated with women’s trust to share mental health problems
Our study provides new insights on where and who women turn to for support on mental health issues. A majority would primarily turn to friends and their spouses. These two groups of people stood out, compared with preferences in turning to other family members or health care professionals. None of the respondents would primarily contact the mother-in-law nor the father-in-law, which is in line with previous research outcomes of interview studies in Shanghai conducted prior to the survey (Schwank et al., 2019b). The women expressed very limited trust in their mother-in-law, who they considered a major source for perinatal mental health problems. The bad well-being group reported that they would distrust their mother-in-law the most and the healthy group distrusted other relatives the most. These findings are in line with findings by Wang and colleagues, whose study analyzed the impact of living with the mother-in-law (Schwank et al., 2019b; Wang et al., 2017). The bad well-being group expressed more distrust in and sought less help from their husband. This finding is in line with previous research describing lower partner support and higher levels of relationship conflict in women with PPD (Dennis and Ross, 2006). Maternal perceptions of social integration and partner provision of problem-focused informational support and positive feedback are important (Dennis, 2005). These findings are in line with our qualitative research, highlighting the protective factor of the husband’s support on the women’s mental well-being (Schwank et al., 2019b). Our study population further reported very little trust in psychiatrists as a primary support with mental health problems (0.2%). This is a critical finding with regard to resource allocation for mental health care services, specifically perinatal mental health care.
Preference for type of professional mental health care
None of the women in this study would turn to a health care professional as a first point of contact, a finding which carries implications for how an improved mental health care infrastructure should be designed. If women consider seeking professional health care, their primary choice would be to visit a community health center. Our findings support the conclusions of Patel and Thornicroft (2009) and the WHO (2015b) “thinking healthy” approach of developing programs for community health workers to provide psychosocial support. This entails emphasizing on mental health services on community level, primary physicians, and non-physician health care providers. Resource allocation on primary care level rather than focusing on education and resources on specialized tertiary hospitals, to which only 5 percent of women in our survey would turn to as a first point of contact. There is an urgent need to improve mental health literacy in primary care staff previously established by Gong and Furnham (2014) and Zhang et al. (2013). With a large treatment gap and underdiagnoses of common mental health disorders, China faces a substantial challenge in mental healthcare, which needs to be addressed (Chisholm et al., 2007; Phillips et al., 2009; Saraceno et al., 2007). This includes a need for increased proficiency of nurses, midwives, and other mid-level practitioners (Ghebrehiwet and Barrett, 2007). A comprehensive policy on mental health would additionally require facing down systematic and cultural hurdles. These hurdles are tied to a central finding in our study, in which women reporting bad mental well-being were less likely than healthy women to seek any help. The lack of help seeking is presenting a challenge in creating systems that can reach those who need help the most (Prince et al., 2007; Zhou et al., 2015).
Attitude toward Internet mental health care services
Our study showed that a majority of the participating women preferred accessing Internet resources for their mental health problems. The preference for seeking help online was equally distributed among both healthy and bad well-being group. These findings are in line with previous qualitative research undertaken by our research group (Schwank et al., 2019a, 2019b). The high proportion of participants expressing a preference for online resources is likely influenced by the stigma associated with mental health problems (Sartorius, 2007). Stigmatization toward mental health issues are found in healthcare providers as well, which further diminishes trust and likelihood to seek help from professionals (Lauber and Rössler, 2007). The well-developed Internet culture in China, with multitudes of ratings and review systems, likely contributes to a higher level of trust in resources which have been vetted by the online community (Huang, 2015).
Strengths and limitations
There are several potential limitations to our study. The study population was restricted to participants from Shanghai, considered both a strength and a weakness. The strength is the focus on one specific area and population in China, with its homogeneous nature. Despite the specific selection criteria of urban women of reproductive age, they belong to the generation of the one-child policy. There are limitations regarding the implications of generalizability to rural China. Recruitment was made using a snowball sampling technique, which imposes limits on representation and reproducibility. The study population hence skewed toward more educated and affluent women, compared with Shanghai’s or the national population. A further limitation is the use of a non-validated tool to assess the women’s global mental health status. Our choice of method provides a preliminary screening rather than an actual mapping of bad mental health among urban Chinese women, and emphasizes self-reported feelings of mental well-being or lack thereof. This choice was made in order to adhere to self-rating scales and the interview guide developed by Chen and colleagues to investigating help-seeking behavior in Urban China (Chen, 2011), and to build on our previous qualitative interview outcomes (Schwank et al., 2019a). The Mainland Chinese validated version of the Kessler Psychological Distress Scale (K10) was deemed suboptimal for our purposes as the examined time frame is short. In addition, previous research using this scale showed a discrepancy between manifestly high self-reported scores and participants despite this not considering themselves as having mental health issues (Chen, 2011, 2012).
Due to opaque regulations and disclosure requirements for WeChat usage, an additional concern may be raised regarding anonymity and perceived lack thereof. It has to be considered how the lack of anonymity might have affected respondents’ truthfulness. Limitations notwithstanding, our study presents strengths in having a sizable sample and using a novel technique and platform. The study population is a good representation of modern, urban women in the prosperous coastal areas of China. Similar sociodemographic characteristics were found in a recent large Shanghai birth cohort study, which support the generalizability of our study further (Zhang et al., 2019). Our findings provide useful information on understanding the development of women’s expectations on help seeking behavior for mental health problems, whom to trust, which professional services to visit primarily, and a clear preference for online resources. The participants were oddly specific about defining the type of online resources they preferred to use. Chinese people depend on their smart phones for most daily activities and use applications such as WeChat to access social media access. However, applications such as WeChat pay or Alipay are also used for most of their daily purchases and transactions. China has one billion WeChat users, tendency rising (CNBC, 2019). We, therefore, consider lack of access to health care professionals and an innate use of smart phones as potential contributors to the large preference of web-based services.
Conclusion
Our study yields insight into urban Chinese women’s care seeking behavior for mental health problems, whom to turn to, trust or distrust, and what form of services they would request. Women from the one-child generation report worse mental health than older generations. Shanghai women avoid seeking help for mental health problems in over 70 percent of all cases, and if they do, they show a clear preference for seeking help online or visiting community health centers. If confronted with mental health problems, they primarily trust friends and spouses. Women who self-report as being in bad mental well-being are less likely to seek any kind of help, and are thus at risk to lack both formal and informal support when needed. There is a call for further investigation with larger cohorts and questions focussing on elucidating the significance behind our current findings.
Relevance for clinical practice
Our results lead us to recommend that decision makers bring attention to challenges faced by the one-child generation, and allocate resources for mental health care on community level. In addition, expand access to online mental health resources. Community health workers and primary care practitioners should be trained in psychosocial support. Services to address spouses should be expanded. Health care providers should be well aware of the potential negative impact on young parents’ mental well-being caused by family members including in-laws. Online resources to support young parents seem to be an excellent way to access the majority of the young couples, and present an unmet need that can and should be filled, by governments and enterprises alike.
Supplemental Material
Appendix_I – Supplemental material for Care-seeking behavior and disclosure on self-reported mental health among young women in urban Shanghai, China
Supplemental material, Appendix_I for Care-seeking behavior and disclosure on self-reported mental health among young women in urban Shanghai, China by Simone Eliane Schwank, Ewa Andersson, Birgitta Wickberg, Shih-Chien Fu, Yan Ding and Helena Lindgren in Health Psychology Open
Footnotes
Acknowledgements
We would like to thank the Shanghai women for their participation in the study and all research staff and clinicians for their hard work that made this study possible. A thank you to the Shanghai Women’s and Children’s Health Center and Chinese American Psychoanalytic Alliance (CAPA) for their great support, and Caroline Raynolds for the English language editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding was provided by the Swedish Foundation for international Cooperation in Research and Higher Education, STINT (grant no. IB2016-6905), and the NSFC.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.