
Abstract
Background
Hidradenitis Suppurativa is a chronic inflammatory skin disease with a strong negative impact on physical and psychological health. Obesity, especially visceral adiposity, but also smoking or unhealthy nutritional habits, have been reported to be significantly associated with hidradenitis suppurativa.
Design and methods
Case-control study in 35 patients of both sexes affected with hidradenitis suppurativa, and 35 healthy subjects matched for sex, age, and geographic origin (Sardinia, Italy).
Results
Several anthropometric measures (body mass index, waist circumference, body composition), lifestyle (Mediterranean diet adherence, and physical activity level), and the perceived physical and mental health status were evaluated in case and controls. Hidradenitis patients showed significantly higher values of body mass index, waist circumference, body composition, fat mass, and lower values of physical and mental health status compared to controls, while both groups showed a similar moderate physical activity level which can be assumed to counteract the negative effects of obesity or poor nutritional pattern in hidradenitis patients. However, none of the evaluated variables were correlated with the severity of the disease, assessed by means of the Hurley stage system or the Sartorius score. Instead, the Sartorius score showed a positive correlation with the duration of hidradenitis, mainly imputable to the diagnostic delay and the consequent long lasting inflammatory status.
Conclusions
Although nutritional factors and lifestyle can be important and modifiable factors in the hidradenitis suppurativa course, the detrimental effect of chronic inflammation and delayed management are clearly prevalent and heavily influence the disease burden.
Keywords
Introduction
Hidradenitis suppurativa (HS) is a chronic inflammatory skin disease also known as acne inversa and, historically, Verneuil's disease, that predominantly affects areas of the folds such as the armpits, groin, perianal, perineal and inframammary.1,2
Significance for public health
The negative impact of Hidradenitis Suppurativa on physical and psychological health is incontrovertibly high, especially in young adults, in the midst of their social and working life. Modifiable negative attitude and lifestyles are an important field of study and intervention, which remain controversial. Although smoking and unhealthy nutritional habits, have been reported to be significantly associated with Hidradenitis Suppurativa, main studies were performed in geographical areas with a high prevalence of obesity. Present case-control study is conducted in a sample of Sardinian population, which confirm a lower obesity rate, a certain relevance of altered anthropometric measures (body mass index, waist circumference, body composition), lower Mediterranean diet adherence, and perceived physical and mental health status in hidradenitis cases. However, none of these factors resulted statistically associated with the severity of the disease, as opposed to the diagnostic and consequent management delay, which confirms is prominent role on the disease burden.
Clinical manifestations range from the development of recurrent inflammatory painful nodules and draining abscesses to the formation of sinus tracts and retracting scars. 3 Due to the discomfort related to its symptoms and signs, especially pain, pruritus, and suppuration, HS is associated with a condition of psychological distress and impaired quality of life.4,5
The prevalence of the disease has recently been reported by 0.7-1.2% in the general European and US population, and females are more frequently affected than males. 6 Onset generally occurs in young adulthood, but a delay in diagnosis and treatment is commonly observed, often related to the patient's reluctance to confide their sufferings to family members themselves, or underestimation of the disease progression (Figure 1), limiting the opportunity windows for effective treatment.7,8 In addition to genetic predisposition (it is estimated that 40% of patients have a relative with HS), several environmental factors, including adiposity and nutrition, contribute to the clinical severity of the HS phenotype. 9
Obesity is known as a major risk factor for HS. Several studies report a positive association between HS severity and body mass index (BMI)10,11 and a recent meta-analysis shows that HS patients are four times more likely to be obese compared to the general population. 12 Overweight or obesity are considered to have a key role in the pathogenesis of HS. In fact, obesity induces a low-grade inflammatory state, characterized by high levels of pro-inflammatory cytokines, and in particular the macrophages that infiltrate the visceral fat produce pro-inflammatory cytokines that exacerbate the activity of HS disease. It has been reported that HS is positively associated with waist circumference (WC), which is considered a marker of visceral adiposity and a better predictor of cardiovascular and metabolic risk compared to BMI. 13 In addition, the excess of weight could favor the onset and worsening of HS due to the excessive friction of the skin on clothes. 14 A recent characterization of HS phenotypes identifies the axillary-mammary- groin phenotype, with predominantly anterior body involvement in obese females, as associated with the most severe symptoms, and limited response to treatment. 15 The exacerbating factors of HS also include smoking habits, and nutrition, especially the role of dairy products or foods containing brewer's yeast.16–18 In addition, a suppressive effect of some micronutrients as zinc gluconate, vitamin D or riboflavin on skin HS lesions has been observed. 19
On the other hand, although weight loss after bariatric surgery has been demonstrated to improve the severity of HS, it was also described a worsening of the disease probably due to the resulting malabsorptive malnutrition. 12 An Italian study, observed in HS patients compared to a control group, a lower adherence to Mediterranean diet (MD), globally recognised as one of the healthiest nutritional models. 20 However, it has been reported that although the nutritional pattern is essential for the maintenance of a healthy status and for the prevention of several diseases, other factors, among which a sedentary behaviour, are equally important, suggesting to introduce the concept of Mediterranean lifestyle instead of that of Mediterranean diet alone. 21
On this background, and in order to further elucidate the relationship between Hidradenitis and obesity or overweight, we aimed to investigate the anthropometric characteristics, the lifestyle habits, in particular the adherence to MD and the physical activity level, and the perception of the state of health in a group of patients with Hidradenitis and in a healthy control group, both resident in Southern Sardinia, also evaluating whether a diagnostic delay of HS could influence the severity of the disease.
Declaration
The study was approved by the Local Ethical Committee as part of the activity of a dedicated epidemiologic registry (Prot.N.21/11/C.E.) and carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans. Written informed consent was signed by the patients or by their parents for subjects younger than 18 years.
Design and methods
A sample of 35 Sardinian patients of both sexes affected with HS attending the outpatients Dermatology Unit of the University Hospital of Cagliari were involved in the study, and referred to the Obesity Unit of the same University Hospital from March 2019 to November 2020.
A control group of 35 healthy Sardinian subjects, matched by sex and age, was recruited among hospital volunteers and students. None of the patients or controls, had followed any specific nutritional program or hypocaloric diet for at least one year. None of the women enrolled in the study reported to be pregnant or breastfeeding. The collected information included demographic and clinical data, anthropometric measures, lifestyle habits, and the health status assessment. In particular, each patient underwent a full clinical evaluation including family and personal medical history, information about smoking, alcohol habits, and drug intake, physical examination and measurement of vital signs. In addition, a blood test comprising routine haemato-chemistry, fasting glucose, and lipide profile was performed.
Regarding HS, the age at onset and the age of first diagnosis were investigated by the dermatologist, who also assessed the severity of the disease by means of the very simple, descriptive Hurley Stage System, 22 and the Sartorius Score, which is a more complex but objective method to quantify the severity of HS, allowing a scale of numerical scores. 23 The Hurley stage system describes three distinct clinical stages, in particular, stage I: single or multiple abscesses, without sinus tracts and scarring; stage II: recurrent, single or multiple abscesses widely separated from normal skin, with initial sinus tract and scars formation; Stage III: diffuse or near-diffuse involvement, or multiple interconnected tracts and abscesses across the entire area. The Sartorius assessment is based on the following criteria: i) the anatomic region involved: 3 points for each region; ii) the number and type of lesions: 2 points for each nodule, 4 points for each fistula, 1 point for each scar, 1 point each for ‘other’; iii) the longest distance between two relevant lesions in each region: 2 points for less than 5 cm, 4 points for less than 10 cm, 8 points for more than 10 cm; or lesion size if only one lesion is present: 2 points for less than 5 cm, 4 points for less than 10 cm, 8 points for more than 10 cm; iv) lesions clearly separated by normal skin in each region: 0 points for ‘yes’, 6 points for ‘no’. The total score is obtained through the sum of the regional scores with an open upper limit.
The anthropometric assessment consisting in the measurement of height and body weight, the calculation of the relative BMI, the measurement of the waist circumference (WC) and the impedance analysis of body composition (BIA) was performed by the same nutritionist as follows: the body weight expressed in kg was measured with an impedance scale (TANITA BC 420), also used for the body composition analysis (fat mass, FM, fat free mass FFM, muscle mass, MM), while the height expressed in cm was measured with a wall statimeter (SECA) consisting of a vertical bar incorporating the meter and a horizontal one to put in contact with the highest point of the head; the BMI was calculated through the ratio between the weight in kg and the height in m2, and used to classify the weight status of the subjects; the WC, expressed in cm, was measured with an anelastic flexible meter on the upper edge of the iliac crests considering the cut-offs of the IDF criteria, 80 cm for females and 94 for males. 24
The lifestyle evaluation was performed by means of validated and standardized questionnaires, administered by the same qualified operators (nutritionist and endocrinologist) during an interview, and included the assessment of the adherence to the Mediterranean diet with the Med Diet Score, 25 the ascertainment of the physical activity level with the IPAQ questionnaire, 26 and the assessment of the state of health, with the SF-12 questionnaire both in patients and controls. 27

A) A 16-year-old boy with initial HS lesions, Hurley stage 1, on the right armpit. B) The patient (who for personal reasons returns to visit 3 years later) with Hurley stage 3 lesion.
The Med Diet Score, considers 11 food groups, and assigns an increasing score from 0 to 5, on the basis of the monthly consumption of foods considered to be close to the Mediterranean pattern, and a decreasing score from 5 to 0, on the basis of the monthly consumption of foods considered away from the same model; the total score, obtained with the sum of the 11 individual scores (one for each food group), ranges from 0 to 55, and higher values indicate a higher adherence to MD.
The IPAQ questionnaire, used in its short form, allows to assess the physical activity level, according to the estimated energy expenditure derived from the reported physical activity (vigorous, moderate and walking) and expressed in Metabolic Equivalent of Taskminutes per week (METs/w). IPAQ allows also to estimate the sedentary behavior, assessing the mean daily sitting time (h/day).
The SF-12 questionnaire (short form survey), the shortened version of the original SF-36 questionnaire, measures both physical (PCS) and mental component (MCS) of the health status; each score ranges between 0 and 100, with a higher score indicating better health.
Statistical analysis
The normality of continuous data was evaluated with the Shapiro-Wilk test. Continuous variables are presented as mean value ± standard deviation (m±SD) or median (range), based on the distribution of the data. Categorical variables are expressed as absolute number and percentage.
A t-test for independent samples was performed to compare the mean scores of anthropometrical measurements and lifestyle factors of patients and controls. Differences in the frequency of sex and smoking status between the two groups were evaluated by Pearson's chi-squared test. Correlation between Sartorius score and patient characteristics was detected by Spearman's correlation. Differences in the Sartorius score between male and female patients were evaluated by the Mann-Whitney U test, while the comparison of patient characteristics between the two sexes was performed by t-test for independent samples. Differences in clinical data in the three Hurley staging (from 1 to 3) of patients, were compared by one-way ANOVA for independent samples. A posthoc analysis was conducted only if the omnibus test was statistically significant. A p-value <0.05 was considered statistically significant for all the analyses performed.
All analyses were conducted using the SPSS statistical package (version 23 for Windows. SPSS, Inc. Chicago, IL, USA).
Results
The study sample consisted of 35 HS patients (22 females and 13 males) with an average age of 30.11±10 years and 35 healthy subjects, matched by sex and age, as control group. No statistical differences between males and females in terms of age were observed both in patients and controls.
The average age of onset of the disease turned out to be 19.5±11.9 years in the whole sample, but males showed an earlier onset compared to females (15.6±8.3 vs 21±13 years; p=0.014). The average age of diagnosis was 27±10.3 years in the total sample, earlier in males than in females (23 vs 30; p=0.014). The mean interval time between onset and diagnosis was in the total sample 8±8.7 years, without any difference between the two sexes (p=0.612). Consequently, also the duration of HS (10.7±7.9 years in the total sample) was similar in both sexes (p=0.780)
The clinical evaluation showed that the localizations of the HS lesions were distributed as follows: genital and inguinal region (88.6%), armpits (62.9 %), buttocks (40%), mammary region (25.7%), trunk (6%).
The severity of the disease, calculated by means of the Sartorius score, revealed, in the whole sample, a median value of 63 (range 23-101), without any significant difference between males (median value = 64; range 26-100) and females (median value = 78; range 25-101) when compared by Mann-Whitney test (p=0.602).
The Hurley Stage System, showed that 8 patients (22,8%) presented with stage 1, 16 patients (45,7%) with stage 2 and 11 patients (31,4%) with stage 3. The percentage of patients diagnosed with stage 3 was higher in males than in females (38.5% vs 27.3%); however, no significant differences were found in terms of frequency of the different stages between the two groups.
The medical history allowed us to detect that, 20 patients (57.1%; 9 M, 11 F) were smokers (at least one cigarette per day) and 15 patients (42.9%; 4 M, 11 F) were non-smokers (p=0.267); with regard to alcohol consumption, this habit was declared by 16 patients (45.7%; 6 M, 9 F), while 19 patients declared to be abstainers (54.3%; 14 F, 5 M). Concerning both these habits, no significant differences were observed between the two sexes (Table 1).
Demographic and clinical data in the whole HS sample and by sex.

HS, Hidradenitis suppurativa.
Regarding clinical data, the mean systolic and diastolic blood pressure values were of 116±19 mmHg and 68±12 mmHg respectively, the mean glycaemic values were 91.4±13.5 mg/dl, the mean triglyceridemia was 95±35.4 mg/dl, the mean cholesterol value was 200±51 mg/dl, while the HDL cholesterol value was 55.7±13.5 mg/dl, without any difference between the two sexes. Based on IDF diagnostic criteria, metabolic syndrome was present in 5 female patients.
The results of the anthropometric evaluation in HS patients are shown in Table 2: the mean body weight was 74.08±15.7 kg (M: 77±14 kg; F: 72.15±16.67 kg) and the mean BMI value of 27.3±6.35 kg/m2 (M: 25.5±5.55 kg/m2; F: 28.3±6.8 kg/m2). No statistically significant differences were observed between the two sexes (p=0.295). According to BMI values, 16 patients (45%; 7 males and 9 females), were classified as normal weight, 8 patients (22.9%; 4 males and 4 females) as overweight and 11 patients (31.4%; 2 males and 9 females) as obese. Overall, 19 patients (54,3%) had an excess of weight. The mean WC value was 89.32±14.8 cm in the total sample, 87.3±14.3 cm in males and 90.04±14.8 cm in females; the average value was higher than the specific sex reference limit (80 cm) exclusively in the female sex. Regarding the body composition, evaluated with the bio-impedance analysis, the mean values of fat mass (FM), fat free mass (FFM) and muscle mass (MM) as well as the mean value of basal metabolic rate (BMR) are reported in Table 2, that shows in male patients a significant higher FFM and MM than in females.
The lifestyle evaluation, consisting of the nutritional analysis and the assessment of the physical activity level by means of the specific questionnaires MDS and IPAQ, showed an average MDS of 26.8±6.4 in the whole sample, with very similar scores in the two sexes (M: 27, 1±7.9; F: 26.6±5.4), while the IPAQ questionnaire, revealed a mean energy expenditure of 1610±1548 METs / week, with a statistically significant difference between the two sexes (M: 2621±247; F: 1012±693; p=0.002); regarding the mean daily sitting time, of 6.7±3.3 hours in the total sample, no significant differences were observed between the two sexes (M: 6.5± .9; F: 6.88±2.9). Finally, the SF12 questionnaire showed similar mean values of the two synthetic indexes, PCS and MCS, in the whole sample (46±10 and 48±11 respectively), without any statistically significant difference between males and females. Lifestyle and SF-12 data are reported in Table 2.
By comparing the group of HS patients with the control group (Table 3), the presence of significant differences in the mean values of BMI, WC, FM, all higher in HS patients than in controls, and in the mean values of MDS and SF-12 PCS, both lower in HS patients than in controls, was observed, as shown in Table 2, whereas there were no significant differences between the 2 groups regarding FFM, physical activity level and SF-12 MCS. Concerning SF-12 MCS, a lower, although not significant value was observed among overweight or obese HS patients compared to normal weight ones. The prevalence of overweight and obesity was significantly higher in HS patients than in controls (p=0.02), among whom, 26 subjects (74.3%) had a normal weight, 9 subjects (25.7%) had a slight overweight, and none of them had an obesity. Moreover, among HS patients there was a significantly higher prevalence of smokers (p=4 × 10−7) than in controls, while, the alcohol consumption, was similar between the two groups.
Anthropometric, lifestyle, and status of health data in the whole HS sample and by sex.

HS, Hidradenitis suppurativa.
Anthropometric, lifestyle and state of health variables in HS patients and controls.
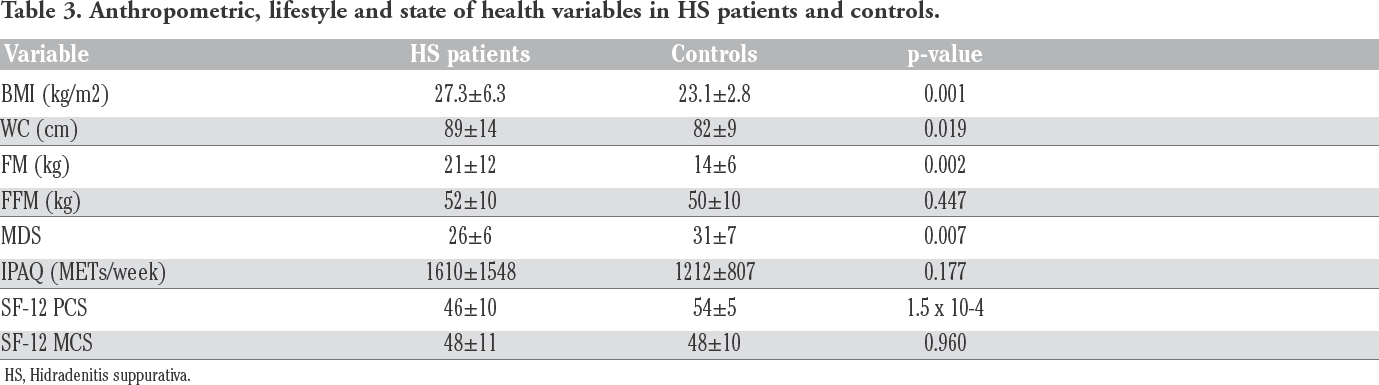
HS, Hidradenitis suppurativa.
On the basis of these results, we investigated the presence of a possible association between the anthropometric characteristics, the lifestyle variables, the heathy status indexes, and the severity of HS, evaluated by means of the Hurley stage system or the Sartorius score. Although clinical impressive differences among patients with increasing BMI index and worsening disease severity index (Figure 2), when we divided the HS patients into three groups, according to the Hurley stages, we did not find any association between the different stages and each of the considered variables. A similar not significant result was observed when we evaluated the Sartorius Score in the HS patients, grouped according to BMI classes, as well as when we analysed the correlation between the different variables and the Sartorius Score. On the other hand, the Sartorius Score was significantly correlated with the duration of HS (Spearman test: p=0.016, R= 0.406), as showed in Figure 3.
Discussion
In our study, patients affected by HS, show significantly higher BMI, WC, and FM values, and a higher prevalence of overweight and obesity, than healthy control subjects matched for sex and age, and coming from the same geographical area (Sardinia, Italy). This finding agrees with the literature data, that highlight the key role of the adipose excess, and especially visceral obesity, in the pathogenesis of HS, despite the variable prevalence of overweight and obesity reported in different studies among HS patients. 28
In this regard, our results differ from those of two other Italian studies, that reported, in HS patients coming from Campania, a higher prevalence of overweight and obesity, and higher values of the anthropometric indexes than those observed in our patients,20,29 probably reflecting the different prevalence of obesity in the general population of the different Italian regions. In fact, Sardinia has one of the lowest prevalence, and Campania one of the highest, especially among children and adolescents. 30 Moreover, in one of the Italian studies aforementioned, the control group also had a high prevalence of obesity. Nevertheless, in the same study, the BIA analysis, showed that HS patients, despite a BMI similar to that of control subjects, presented several alterations in body composition not observed in controls, but associated to the severity of HS, and suggestive for an inflammatory state. 20
Chronic inflammation represents the central component in the pathophysiology of the skin lesions of HS. The natural characteristics of the skin areas involved, the high temperature and moisture, the reduced oxygen availability, and the specific microbiome composition, favor the development of the inflammatory process that starts in the perifollicular area, and subsequently determines the occlusion and dilatation of the hair follicle unit. The resulting bacterial growth with the particular increase of the anaerobic taxa, and the release of damage-associated molecules, induce the activation of local macrophages, the secretion of pro-inflammatory cytokines, and the infiltration of immune cells, especially neutrophilic granulocytes, worsening the inflammation process, and finally leading to the destruction of the hair follicle unit. 31
Obesity, body composition alterations, and particularly visceral adiposity, are also characterized by a low-grade chronic inflammation, with the production of pro- inflammatory cytokines such as IL- 1β and TNF-α, and are considered major contributors to the development of HS. 3 . Central obesity and metabolic syndrome have been reported in a large proportion of HS patients, even before the diagnosis of HS. 33 Among the environmental factors involved in the pathogenesis of obesity and its complications, lifestyle is fundamental, and several studies investigated its role in HS patients. In particular, it have been highlighted the role of tobacco smoking and the effect of nicotine on the skin 34 , and a high prevalence of smokers has been found among HS patients.35,36
Another field of interest, is represented by the evaluation of the dietary patterns in HS patients, and a negative role of some components of diet, such as dairy food 37 or brewer's yeast 38 has been hypothesized. In the study of Fernandez et al., a sample of HS patients was asked, by means of an anonymous questionnaire, to indicate foods that respectively exacerbated or alleviated HS symptoms; among the former, were indicated sweets, carbohydrates, dairy and high-fat foods, while among the latter, were indicated vegetables and fruits, chicken and fish. 39
Mediterranean diet, characterized by a high intake of vegetables, fruit, legumes, wholegrains and fish, and by a low intake of meat and dairy, is considered one of the healthiest nutritional models, and due to its richness in antioxidants compounds, such as polyphenols, contained in plant-derived food, it has considered to have a protective role against both inflammation and obesity, as well as to modulate the gut microbiota composition in obese patients.40–42
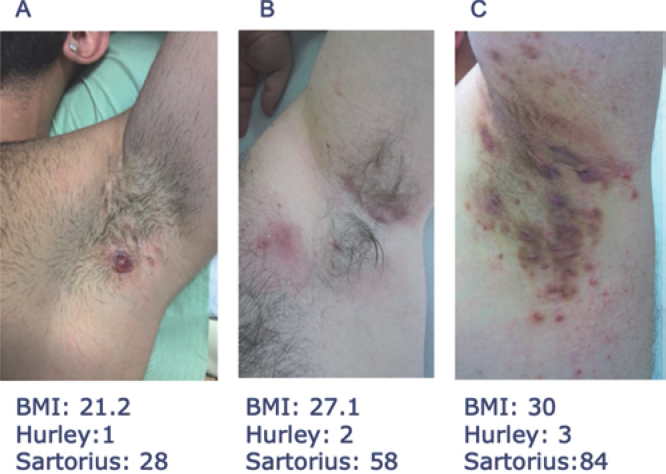
Increasing BMI and HS severity staging in 3 different male patients, with lesions on the same body area.

Spearman Correlation between Sartorius score and duration of HS.
In HS patients, a low adherence to the Mediterranean diet has been observed, and in detail, a nutritional pattern characterized by an excess of simple carbohydrates and saturated fats, and a low intake of complex carbohydrates, fiber, mono-unsaturated and n-3 poly-unsaturated fats has been described. Moreover, in the same study, the degree of adherence to Mediterranean diet, has been shown to be negatively associated to the severity of HS. 20 In line with the literature, we found a significantly higher proportion of smokers among HS patients, compared to healthy subjects. Moreover, HS patients showed a significantly lower adherence to the Mediterranean diet than that of controls. Altogether, these results are indicative of an unhealthy lifestyle.
In addition to eating habits and nutritional patterns, the other fundamental aspect of lifestyle is physical activity. The negative impact of the sedentary behavior on general health, 43 and the crucial role of physical activity in the prevention and treatment of obesity and non-communicable diseases44,45 have been well established. However, there is no data about this aspect in HS patients. An accurate estimate of energy expenditure requires a complex, and also expensive evaluation. 46 The short form of IPAQ is a simple, but reliable and valid tool for assessing and monitoring the physical activity level. 26 We assessed, by means of IPAQ, the physical activity level in our study population, obtaining similar results in HS patients and in controls. In contrast to dietary habits, significantly worse in patients than in controls, both groups showed a moderate physical activity level and a comparable daily sitting time. We therefore investigated the possible association between the anthropometric indexes or the lifestyle aspects and the severity of HS, evaluated both with the Hurley Stage System and the Sartorius Score, but we did not find any significant result.
This finding is in contrast with other studies, that reported an association between BMI values,47,48 BIA alterations or Mediterranean diet adherence, 20 and the Sartorius score. A possible explanation is that in our HS patients, the moderate physical activity level, similar to that observed in healthy controls, could exert a protective effect on health, counteracting the negative impact of the other factors, and particularly the poor eating habits. In fact, it has been demonstrated, that regular physical activity may help in maintaining or losing weight, as well as in improving the metabolic alterations associated to overweight or obesity, such as insulin resistance, lipid disorders and hypertension. In addition, aerobic exercise has shown to reduce inflammation. 49
Our HS patients’ group, although having higher BMI and WC values than the control group, showed, a mean WC value not particularly high. Moreover, considering the two sexes separately, we observed that the WC mean value, exceeded the cut-off value exclusively in females, who had a physical activity level significantly lower than males. In addition, male patients showed a better body composition than females, with lower, although not significant, BMI and FM values, and significantly higher FFM and MM values, all attributable to a more active lifestyle. Furthermore, the few patients who showed clinical data compatible with the diagnosis of metabolic syndrome, were all females.
Finally, despite the not significant result, in our patients, even the Sartorius score showed a lower trend in males than in females. Unlike the results obtained with the other variables, we found a significant correlation, between the Sartorius Score and the duration of HS. Considering that the duration of HS comprises also the period preceding the diagnosis of the disease, we hypothesized that the diagnostic delay has had a strong impact on the clinical severity of HS. An average diagnostic delay of more than seven years has been reported worldwide 50 and our results are in line with this data. Moreover, our results also agree with those obtained by Kokolakis et al., who in a cohort of German HS patients, reported an association between the diagnostic delay and the severity of HS, by means of the Hurley Stages system. In that study, an increased number of comorbidities linked to the inflammatory status, and an impairment of the patient's professional life were also associated to the diagnostic delay. 51 A similar result was found by Omine et al., in Japanese HS patients, in whom the severity of the disease evaluated with the Sartorius Score, correlated with the duration of the disease. 52 Interestingly, as in our study, the researchers did not find any association between the Sartorius score and the BMI value, which indeed, showed, in Japanese patients, a mean value similar to that observed in our patients.
Furthermore, we evaluated the perceived state of health, by means of the SF-12 questionnaire, obtaining in HS patients, compared to controls, a significantly lower physical score, but a superimposable mental score. It has been reported that HS, due to its disabling clinical features, has a strongly negative impact on health and quality of life, 53 and in a recent study performed on an Italian HS cohort compared to a representative sample of the Italian general population, it has been observed a worse score of both physical and mental health status evaluated with the SF-36 (in patients) or the SF- 12 (in controls) questionnaire. In particular, the authors reported that young HS patients, even if affected by a mild or moderate form of the disease, showed scores similar to those of older controls. 54 Moreover, the same group of researchers, reported that the level of pain was associated with the clinical severity of HS. 55 This finding is partially in contrast with our results, that did not show, a significant association between the physical score, that includes the perception of pain, and the Hurley or the Sartorius scores. Hidradenitis has been also associated to a poor mental health, with a high frequency of anxiety and depression, and a negative impact on quality of life. 56 In our study, we obtained in HS patients a mental score not significantly different than that observed in the control group, with a mean value only slightly lower in HS patients classified as Hurley stages 2 or 3 compared to those classified as stage 1. In this regard, our results agree in part with those of the group of Sampogna et al., who showed that the severity of HS was not associated to depression, despite an important frequency of depression among HS patients. 57 Finally, a slightly, but not significantly lower MCS mean value, was found in HS overweight or obese patients compared to normal weight HS patients, probably due to the involvement of psychopathological factors in obesity.58,59
This study has some limitations. First of all, the small number of HS patients, that could have limited the power of the statistical analysis. Unfortunately, the recruitment phase fell into the prolonged lockdown period consequent to the COVID-19 pandemic in Italy, and the general measures to limit the access to the hospitals for not urgent cares. Controls were recruited among volunteers and students, to be matched with patients’ demographics. Another limitation is in the cross-sectional, non-interventional design of the study, which did not allow the evaluation of the potential effects on the severity of HS, of some modifiable lifestyle factors, such as the adherence to the Mediterranean Diet, that might be modified through the adoption of an appropriate nutritional program. In addition, the BIA analysis, performed with a BIA scale, did not allow to determine some variables of the body composition, such as the phase angle, that in previous studies resulted to be altered in HS patients. Finally, the study population included both naive and treated patients, and because of the different therapeutic approaches, the possible impact of the specific treatment on the severity of the disease was not evaluated.
Conclusions
In line with other studies, our HS patients show a higher prevalence of overweight and obesity in respect to healthy controls, both of Sardinian origin, despite an overall prevalence of obesity lower than esteems reported from other Italian regions. Moreover, among HS patients, compared to controls, we found a higher proportion of smokers, worse eating habits and an impaired perceived physical health status, highlighting the importance of the systematic evaluation of the many factors behind body mass index. Surprisingly, we found no statistically significant association between all these altered lifestyle components and the severity of the disease. A possible explanation is that maintained levels of physical activity, which in our HS patients did not differ from controls, might exert a positive, protective effect against the other unhealthy lifestyle factors. Instead, the finding of a significant association between the Sartorius score and the disease duration confirms the negative prognostic influence of the diagnostic delay, and the detrimental effect of the chronic inflammation.
Footnotes
The authors declare that they have no competing interests, and all authors confirm accuracy.