
Abstract
Background:
Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by persistent patterns of inattention and hyperactivity. It affects both children and adults, including university students, and is associated with their academic and functional impairments.
Aims:
This study mainly aims to estimate the prevalence of ADHD among university students and explore its associated factors, including sleeping hygiene, physical activity, dietary habits, and psychological well-being.
Design and methods:
This study utilized a cross-sectional design among university students at AN-Najah National University in Palestine. Data were collected through an online questionnaire, which included sociodemographic and medical history. Lifestyle was evaluated using the sleeping hygiene index (SHI) for sleeping quality and the international physical activity questionnaire-short form (IPAQ-SF) for physical activity. The Mediterranean diet adherence screener (MEDAS) was used to assess participants’ adherence to the Mediterranean diet. For psychological well-being evaluation, the general health questionnaire-12 (GHQ-12) was used. While the adult ADHD self-reported scale (ASRS) was utilized for ADHD screening.
Results:
A total of 402 undergraduates were included in the final analysis. Within the sample, 85.1% were female, and 29.6% were reported to have positive probable ADHD. Univariate analysis revealed that ADHD symptoms were significantly associated with having chronic diseases (p = 0.002), younger age, poor sleeping hygiene, and poor mental health (p < 0.001). Multivariate analysis indicated that age, sleeping hygiene, psychological well-being, and chronic diseases are significant predictors of ADHD (p < 0.05).
Conclusions:
Probable ADHD showed a notable prevalence among university students and is associated with sociodemographic, lifestyle, and mental health factors, underscoring the importance of comprehensive support systems within educational instuitions.
Introduction
Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by persistent patterns of inattention, hyperactivity, and impulsivity that significantly impair the daily functioning and quality of life of individuals with ADHD. 1 The etiology of ADHD is diverse, and many factors are associated with ADHD incidence, including environmental factors such as preconceptional, gestational, and perinatal conditions, as well as heavy metal exposure. Furthermore, genetic factors are associated with ADHD in which many genes are involved in ADHD and participate in processes like neurotransmission, neuritogenesis, and synaptogenesis. 2 In addition, sleep disorders or deprivation, either acute or chronic, are found to be related to reduced cognitive functioning, which is one of the main traits of ADHD patients that can produce significant impairments in attention, mood, and behavior. 2 However, evidence proposes that ADHD is linked with many other individual factors, including physical activity, screen time, and dietary patterns. For instance, a high-quality diet like the Mediterranean diet may have a protective effect against ADHD, while a poor-quality diet accompanied by reduced sleep and physical activity can be associated with an increased risk of ADHD. 3
However, although ADHD was previously believed to be a condition that only affected children, it is now recognized as a persistent condition for a significant proportion of adults who meet ADHD diagnostic criteria. 4 Current estimates indicate a global prevalence of ADHD ranging between 5.9% and 7.1% among children and 1.2% and 7.3% in adults. 1 According to the Diagnostic and Statistical Manual version 5 (DSM-5), adults with ADHD, including university students, often exhibit typical characteristics such as inattention, hyper-attentiveness, disorganization and forgetfulness, hyperactivity, restlessness, fidgetiness or having lots of energy, impulsivity, and emotional lability. 5
Research indicates that ADHD in university students is associated with significant academic and functional impairments. Evidence has reported that university students with ADHD receive lower grades, have poorer study habits, experience difficulties completing tests and assignments on time, engage in fewer study skills, make slower progress in their programs, and are more likely to withdraw from classes and persist for fewer semesters in their programs when compared to their peers without ADHD. 6
Given the considerable impact of ADHD on university students and the importance of understanding its associated factors, this study mainly aims to estimate the prevalence of ADHD probability among university students, as well as explore its associated factors, including sleeping hygiene, physical activity, dietary habits, and psychological well-being. The findings of this study will help understand the multifactorial nature of ADHD and can be used in a targeted intervention to improve the quality of life of university students with ADHD.
Methods
Study design and population
A cross-sectional design was utilized in the present study. The sample size was calculated using a proportion for a finite population. The sample size was determined using Open Epi software, with an alpha of 0.05 (two-sided) and 80% power (beta = 0.2). The effect size was calculated based on a previous study that reported a 26% prevalence of ADHD among Saudi university students. 7 To estimate sample size, we assumed a 10% difference in prevalence compared to our target population. A minimum of 339 participants was necessary to determine the prevalence of ADHD. Furthermore, the sample size calculation considers the goal of determining the relationship between ADHD and mental health, lifestyle, and sociodemographic characteristics. For sample size estimation, a moderate effect size of Cohen’s d of 0.5, a level of significance or type I error of 0.05 (5%), and a power or type II error (1−β) of 0.8 (80%) were used. The sample size calculations all indicated that a minimum of 400 individuals would be sufficient to conduct the analyses. Given the dropout owing to missing data, the sample size was increased to include at least 430 participants.
The study was conducted at An-Najah National University in Nablus City, West Bank, which is one of the largest universities in Palestine. It enrolls approximately 25,000 students across 11 faculties located throughout five different campuses, offering 128 bachelor’s degree programs, 78 master’s programs, and 13 PhD programs. 8
Participants who were included in this study are An-Najah University students who were at least 18 years old. Exclusion criteria included postgraduate students and individuals who were previously diagnosed with ADHD by a specialist.
Ethical consideration
This study was conducted in accordance with the Declaration of Helsinki. The Institutional Review Board (IRB) ethical committee of An-Najah National University approved the study protocol (Reference number: Agr. Vmed. Dec. 2024/3). Electronic informed consent was obtained from all eligible participants prior to completing the online survey.
Data collection and research tools
Data was collected from 15 November 2025 to 25 December 2024 using an online questionnaire, which consists of five parts and was developed using Google Forms and shared online through platforms commonly used by university students, including WhatsApp groups and official faculty social media platforms. The first part discusses sociodemographic data (age, sex, living area, and marital and working statuses), medical history, including chronic diseases and regular medication (any medications taken routinely for any purpose, including medications for chronic conditions, supplementations, or any other reason), and data related to faculty name (including Faculties of Agriculture and Veterinary Medicine, Engineering and Information Technology, Medicine and Health Sciences, Business and Communication, Humanities and Educational Sciences, Fine Arts, Science, Shari’ah, and Law and Political Sciences), and academic grade. The second part focuses on lifestyle, including the Sleeping Hygiene Index (SHI) to evaluate sleeping quality and the International Physical Activity Questionnaire Short Form (IPAQ-SF) to assess the physical activity level among participants. The third part includes nutritional habits-related data (contains questions about breakfast, meal and snack frequency, and caffeine intake), height and weight, and adherence to the Mediterranean diet using the Mediterranean Diet Adherence Screener (MEDAS). The fourth part evaluates psychological well-being using the General Health Questionnaire-12 (GHQ-12), while the last part contains the adult ADHD self-report scale (ASRS).
Sleeping Hygiene Index (SHI)
The validated and reliable Arabic version of SHI was used in this study. 9 The SHI is a self-reported 13-item instrument used to assess sleep hygiene behavior during day-to-day life. In this study, a dichotomized scoring system was employed for each item (no = 0, yes = 1). The items were summed to obtain a total SHI score ranging from 0 to 13. A higher score indicated poorer sleep hygiene. 10
The International Physical Activity Questionnaire short form (IPAQ-SF)
The short version of the International Physical Activity Questionnaire (IPAQ-SF) was utilized to analyze participants’ physical activity levels. The IPAQ-SF is a 7-item questionnaire. In the first six questions, participants were asked about the frequency and daily cumulative time of physical activity in the past 7 days from the aspects of high-intensity PA, moderate-intensity PA, and walking. The last question asked about the sitting situation.11,12 The results were categorized into three levels: low activity (individuals who did not meet criteria for moderate or high categories), moderate activity (≥3 days of vigorous-intensity activity of at least 20 min per day; ≥5 days of moderate-intensity activity and/or walking of at least 30 min per day; or 3–5 or more days of any combination of walking, moderate-intensity or vigorous-intensity activities achieving a minimum total PA of at least 600 MET-min/week), or high activity levels (vigorous activity on at least 3 days with a minimum total PA of at least 1500 MET-min/week or 7 days of any combination of walking and moderate- or vigorous-intensity activities with a minimum total PA of 3000 MET-min/week). 13
Mediterranean diet adherence screener (MEDAS)
MEDAS is a 14-item scale designed to measure the degree of adherence to the Mediterrnean diet (MD), which is an extended version of a nine-item scale. The validated Arabic version was used in this study. It includes 12 questions on food frequency and two on dietary habits, with each question scoring 0 or 1. 14 The final MEDAS score can range between 0 and 14. For categorization of the adherence to the MD, we applied the following criteria: weak adherence, ≤5; moderate to fair adherence, 6–9; good or very good adherence, ≥10. 15
Although Mediterranean Diet adherence and physical activity levels were categorized into low, moderate, and high based on established clinical thresholds to facilitate interpretability and applicability in public health contexts, both variables were also analyzed as continuous variables (MEDAS score and IPAQ-SF score, respectively) to preserve statistical power and capture more nuanced associations.
The General Health Questionnaire-12 (GHQ-12)
The general health questionnaire is a 12-item validated and reliable tool for general screening to measure minor psychological distress. 16 The Arabic version of GHQ-12 was used in this study, which has a Cronbach alpha of 0.86. 17 Likert scoring was used for the rating scale in this study, which ranges from 0 to 3, where zero represents the healthiest and 3 represents poor health/illness, and the total score can range from 0 to 36. 18 A score exceeding the threshold value of 16 was classified as having mental distress. 19
The Adult ADHD Self-report Scale (ASRS)
The ASRS is a self-reported screening scale that includes 18 items that correspond to the DSM-IV criterion for ADHD. 20 The responses regarding symptom frequency utilized a five-point Likert scale ranging from never (0), rarely (1), sometimes (2), often (3), to very often (4). The total sum ranges from 0 to 72. Optimal scoring in the original English version was maintained through unweighted dichotomous responses, independently for each item, 21 that is, ratings of “sometimes,” “often,” or “very often” on items 1–3, 9, 12, 16, and 18 are assigned one point (ratings of “never” or “rarely” are assigned zero points). For the remaining 11 items, ratings of “often” or “very often” are assigned one point (ratings of “never,” “rarely,” or “sometimes” are assigned zero points). 22 Using this scoring method, cut-off scores of ≥9 (range 0–18) for positive ADHD symptoms. 21 In this study, the ASRS was used in the Arabic version after the back translation, and a pilot study was conducted among 30 students for a reliability test, which utilized a Cronbach’s alpha of 0.93.
Statistical analysis
Data was analyzed using the statistical package for the social sciences (IBM-SPSS) statistical software version 28. Continuous variables were analyzed using descriptive statistics such as means and standard deviation, while categorical variables were described using percentages and frequencies. To investigate the relationship between continuous and categorical variables, the Chi-square or independent sample t-test was used where appropriate. The level of significance was set at a p-value < 0.05. Further analysis was performed using a binary logistic regression model, and the logistic regression assumptions were checked before conducting the analysis. The multicollinearity was checked using collinearity diagnostic tests. The Hosmer-Lemeshow goodness-of-fit test was employed to assess how well the model fits the data.
Results
Participants’ recruitment
Figure 1 shows participant recruitment steps. A total of 436 university students, who met the inclusion criteria and gave their consent to participate, were included in the study, and 402 undergraduates were included in the final analysis.

Recruitment steps of undergraduates participants.
Sociodemographic and medical history characteristics
Table 1 presents the characteristics of the analyzed participants. The mean age was 21.08 ± 2.09 (18–30) years. The majority of them were females (85.1%), single (87.1%), living in a village or camp (60.7%), studying in the Faculty of Agriculture and Veterinary Medicine (39.1%), and had a good GPA (46.0%). A minority of study participants are working (9.5%) and having chronic diseases (5.0%), including asthma (1.2%), irritable bowel syndrome (1.0%), hypothyroidism (0.7%), and diabetes (0.5%). In addition, 7.7% are taking medications on a regular basis.
Sociodemographic and medical history of study participants presented in N (%) or mean ± SD.

Note. Only 1.7% of participants reported residing in refugee camps. Most of the sample were from urban or suburban areas in or around Nablus City.
The percentage of participants reporting regular medication use (7.7%) is slightly higher than those reporting chronic diseases (5.0%) due to the use of medications for non-chronic conditions, such as supplementations, contraceptives, and treatments for acne or dermatological conditions.
Lifestyle characteristics: physical activity and sleeping quality
Most study participants, using IPAQ-SF, were presenting a low level of physical activity (275 (68.4%)), followed by a moderate level of physical activity (99 (24.6%)) and a high level of physical activity (28 (7.0%)), as illustrated in Figure 2. Regarding sleeping quality among students, the mean score of the sleep hygiene index was 7.04 ± 2.73 (0–12).
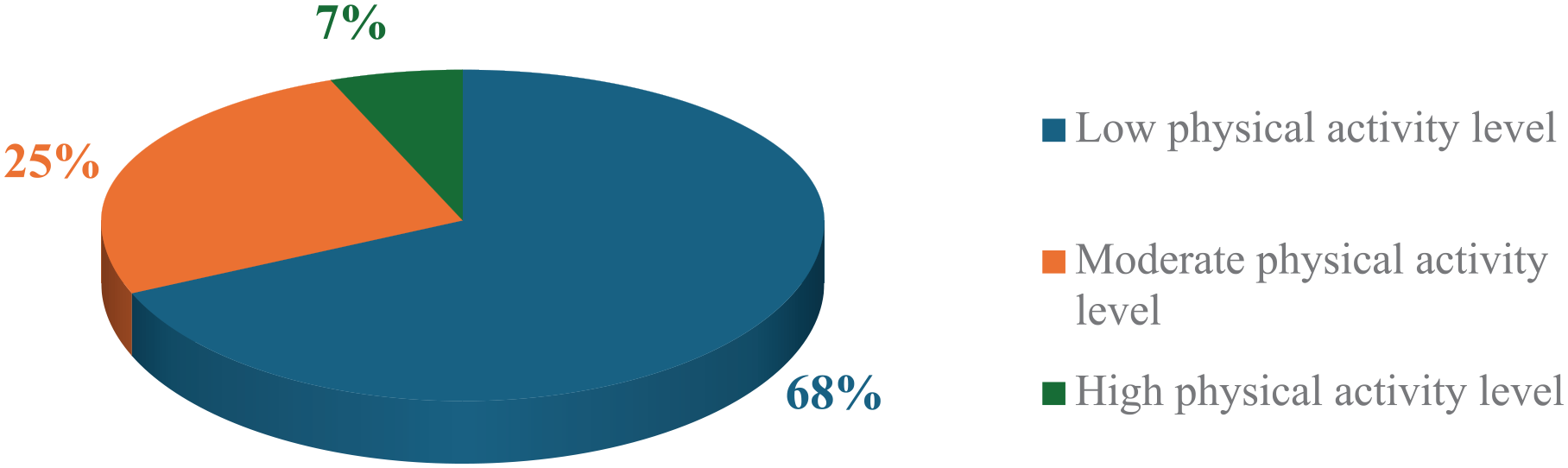
The percentage of physical activity level according to the IPAQ-SF.
Nutritional and mental health characteristics
Most of the study participants are having two main meals per day (59.0%), while 41.8% are having two snacks. 45.8% sometimes have breakfast, and caffeinated drinks were consumed by 80.3% of students participating in this study, as presented in Figure 3(a).

(a) Frequency of daily eating habits. (b) Levels of adherence to the Mediterranean diet as assessed by MEDAS.
According to the MEDAS score, the majority of students are showing moderate to fair adherence to the Mediterranean diet (60.4%), as illustrated in Figure 3(b). The most followed components of the MD were using olive oil as the main source of fat for cooking (80.8%), consuming more than two servings of vegetables, pasta, rice, or other dishes seasoned with sofrito per week (79.6%), and consuming at least three servings of nuts (including peanuts) per week (67.2%). On the other hand, low adherence was observed in the intake of at least three servings of fish or seafood and legumes per week, reported by 11.7% and 21.1% of participants, respectively. The MEDAS mean score was 6.98 ± 2.41 (0–14), and the mean BMI was 23.27 ± 4.49 (10.46–60.61) kg/m2.
Regarding participants’ mental health, the mean score of GHQ among university students was 13.43 ± 5.31 (0–32), with 98 (24.4%) representing a GHQ score > 16.
Self-reported ADHD
The mean score of the adult ADHD scale was 30.95 ± 8.93 (0–54). Within the sample, 29.6% (n = 119) of the participants reported having significant symptoms of inattention or hyperactivity or both, indicating probable ADHD, as shown in Figure 4.

Prevalence of ADHD based on the ASRS screening results.
Association between ADHD and study variables
Among sociodemographic characteristics, only age was found to have a significant association with probable ADHD among study participants (p < 0.001), as analyzed in Table 2. Chronic diseases were significantly associated with probable ADHD (p = 0.002). Regarding lifestyle characteristics, the SHI score was significantly associated with probable ADHD (p < 0.001). However, the GHQ score has shown a significant association with probable ADHD among study participants (p < 0.001; Table 2).
The relationship between study variables and probable ADHD.

Note. The “Health and Medicine” category includes the Faculty of Medicine and Health Sciences. The “Human Sciences” category includes the Faculties of Business and Communication, Humanities and Educational Sciences, Fine Arts, Shari’ah, and Law and Political Sciences. The “Natural Sciences” category includes the Faculties of Agriculture and Veterinary Medicine, Engineering and Information Technology, and Science.
Significant at *: p < 0.05, **: p < 0.001 according to independent sample t-test or Chi-square test.
ADHD predictors
The binary logistic model included the significant predictors found in the univariate analysis (age, SHI score, GHQ score, and chronic diseases). The Hosmer-Lemeshow test for the final model showed that the goodness of fit of the model was acceptable (p = 0.275); Cox & Snell R square was 0.184; and Nagelkerke R square was 0.261. According to this model, age, SHI score, GHQ score, and chronic disease are predictors of probable ADHD (p < 0.05), that is, younger age (Exp(B) = 0.803, p < 0.05, 95% CI = 0.697–0.926), higher SHI score (Exp(B) = 1.197, p < 0.05, 95% CI = 1.082–1.324), higher GHQ score (Exp(B) = 1.111, p < 0.05, 95% CI = 1.065–1.172), and chronic diseases (Exp(B) = 3.790, p < 0.05, 95% CI = 1.272–11.292) increase the risk of ADHD, as shown in Table 3.
Predictors of probable ADHD using binary logistic regression analysis.
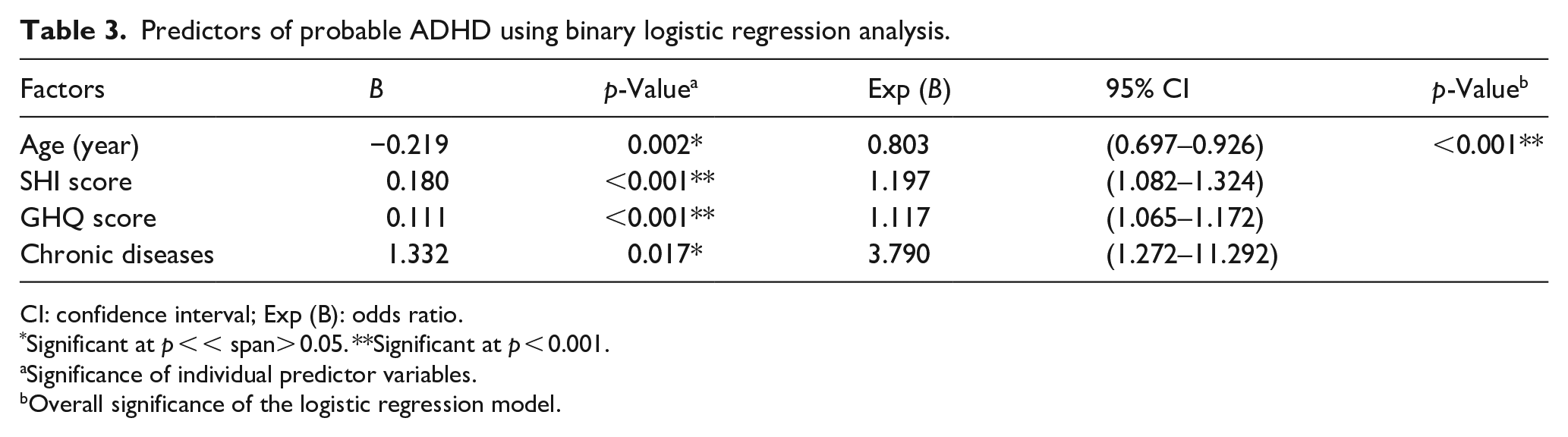
CI: confidence interval; Exp (B): odds ratio.
Significant at p < < span> 0.05. **Significant at p < 0.001.
Significance of individual predictor variables.
Overall significance of the logistic regression model.
Discussion
The findings of the current study revealed that there is a relatively high rate of probable ADHD among undergraduates in Palestine. Notably, approximately 30% of undergraduates reported having symptoms of inattention or hyperactivity, indicating a probable ADHD. This is higher than the global population average of ADHD reported among adults (3.3%), based on 49 two-stage clinical studies, according to a recent meta-analysis. 23 However, our findings align with studies in neighboring countries. For instance, a study in Egypt found that 35% of medical university students met the criteria for probable ADHD based on ASRS. 1 Another study in Lebanon reported that 24.2% of university students showed possible ADHD symptoms. 24 The high prevalence of ADHD symptoms in this study might be attributed to the tool itself, which indicates the probability of ADHD rather than providing a formal diagnosis, as well as the young age of university students, as evidence suggests that ADHD is more common in younger adults. 1 In addition, it might be related to underlying biological, cultural, and familial factors, 25 resulting in higher prevalence rates of ADHD symptoms among undergraduates participating in this study. Furthermore, the high prevalence of ADHD symptoms might be because the ASRS cut-off score has not yet been formally validated or culturally adapted for the Palestinian population, highlighting the need for future research to validate the ASRS within this specific population. Moreover, it’s worth noting that the sociopolitical condition of the Palestinian community might be a contributing factor in the high prevalence of ADHD-like symptoms. Recent research highlights the connection between political socialization, psychological resilience, and post-traumatic stress disorder among the Palestinian people amidst the arduous adversities they face. 26 Another study conducted among undergraduates from three Palestinian universities, including An-Najah National University, revealed that political violence often leads to symptoms of depression and anxiety among undergraduates, 27 each of which underscores the psychological consequences of interaction between individuals and occupying forces and reminds us to consider chronic stressors, which may have influenced the expression and mimicry or intensified ADHD symptoms among our study participants. However, further investigations are required in this regard.
In studying factors associated with ADHD, younger age was more associated with probable ADHD among university students, and younger age was a significant predictor of ADHD in the current study. The association between ADHD and younger age is consistent with findings from other studies. Buźniak et al. found that hyperactivity symptoms decrease with age. 28 Another study in Saudi Arabia found that the prevalence of ADHD among younger students (<20 years) was higher than the prevalence among older students. 7
Interestingly, we found a significant difference between students with and without ADHD symptoms regarding chronic diseases. Students having chronic diseases showed a higher prevalence of ADHD symptoms, while multivariate analysis revealed that having a chronic disease is a significant predictor of probable ADHD symptoms. Our results are in agreement with previous findings in which a significant association was found between ADHD among adults and several somatic diseases, including hypothyroidism, asthma, and irritable bowel syndrome, 29 which are the predominant diseases among our study participants. However, due to the incomparable data set regarding the types of chronic disease, we were unable to explore their direct relationship with ADHD among adults. Still, this could be considered for future studies.
In the current study, poorer sleeping quality was significantly and highly associated with probable ADHD. In addition, poor sleeping quality was a significant predictor for ADHD. These findings are in line with results from recent studies, which showed a high prevalence of sleep disorders in adult subjects with positive probable ADHD, with a high rate of moderate and severe sleep disorders.30,31 ADHD and sleep disturbances in young adults were associated due to genetic and non-shared environmental influences, according to previous literature. 32
When analyzing mental health among students who participated in this study, the GHQ score was positively associated with probable ADHD, suggesting a significant relationship between poor psychological well-being and probable ADHD. Similarly, previous studies found that ADHD symptoms were associated with lower levels of mental health, 33 in which ADHD symptomatology was inversely linked to subjective well-being among university students. 34
This study has several limitations, including the cross-sectional design that limits casual effect relationships, the sample was collected using convenient sampling via an online Google form, which may introduce selection bias, and the study was conducted at a single university, which may affect the generalizability of the findings. In addition, the self-reported data may introduce recall bias, and the high percentage of female participants may limit the applicability of the results. Despite these limitations, this study has strengths, including the comprehensive data collection with a diverse range of measured variables, the use of validated assessment tools, and a relatively large sample size.
Conclusion
To conclude, this study found that 30% of university students have probable ADHD, highlighting a notable prevalence of ADHD symptoms among university students in Palestine. Findings reveal that younger age, chronic diseases, poor sleeping quality, and poor mental health are significantly associated with ADHD symptoms among university students and considered as significant predictors for probable ADHD. The findings of this study are valuable for developing targeted intervention programs to support individuals with ADHD symptoms, particularly university students.
Footnotes
Acknowledgements
The authors would like to acknowledge the students who participated and agreed to join the study.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki. The Institutional Review Board (IRB) ethical committee of An-Najah National University approved the study protocol [Reference number: Agr.Vmed. Dec. 2024/3].
Consent to participate
An electronic informed consent was obtained from all participants prior to completing the online survey.
Author contributions
The authors have contributed to the manuscript as follows: M B: the principal investigators optimized the study proposal and protocol, supervised the data analysis, and edited the final manuscript file. F A: analyzed the data and wrote the final draft of the manuscript. S Q, M D, M D, and Y S: drafted the study proposal, applied for ethical approval, data collection, and data entry. All the authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.